
04-12-2024
This is an online E Log Book to discuss our patient's de-identified health data shared after taking her signed informed consent. Here we discuss our patient's problems through series of inputs from available global online community experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.
PPM 1 - 
Afternoon session: 67F ICU 2 shifted on a ventilator, currently on T piece
Striking cerebral ptosis with bilateral eyes closed!
Inclusion criteria for cerebral ptosis were as follows:
1) sudden bilateral lid drop within 48 hours of stroke,
2) voluntary, spontaneous, and automatic impairment in eyelid opening,
3) preserved voluntary frontalis muscle contraction, and
4) neuroradiological evidence of supratentorial ischemic or hemorrhagic damage.
The exclusion criteria were presented together to distinguish the following causes of ptosis: apraxia of lid opening (ALO), impaired consciousness, blepharospasm, intrinsic oculomotor dysfunction, neuromuscular disease, brain stem dysfunction, and subtentorial lesions.
05-12-2024

PPM 1 - Updated fever chart.
@PPM3 sepsis too 10 days of community acquired sepsis? UTI followed by AKI followed by hypoglycemia followed by rmca infarct followed by cerebral ptosis.

PPM 1 - @PPM4s flawless history.
PPM 1 - 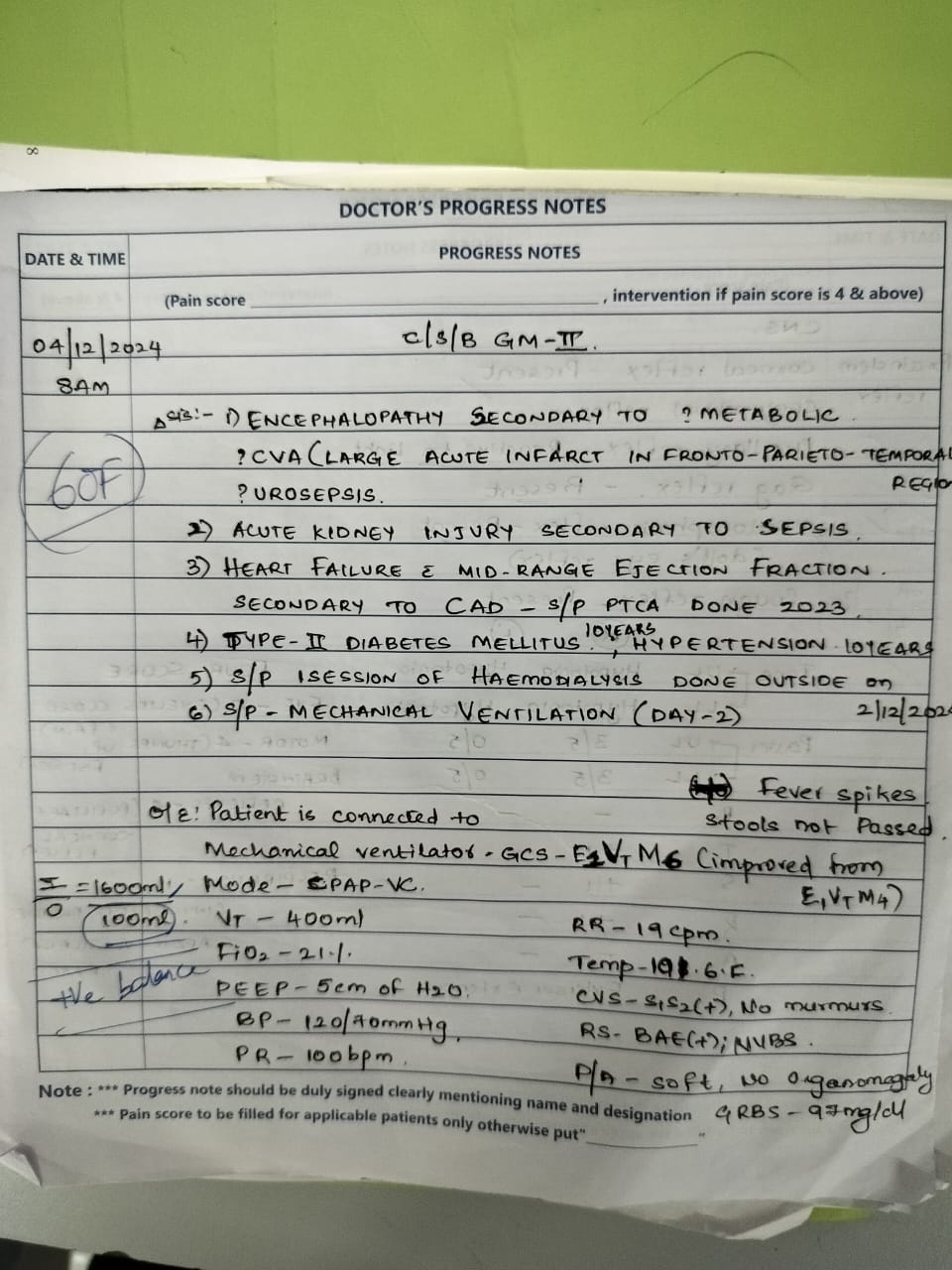 Yesterday's notes by @PPM5
Yesterday's notes by @PPM5
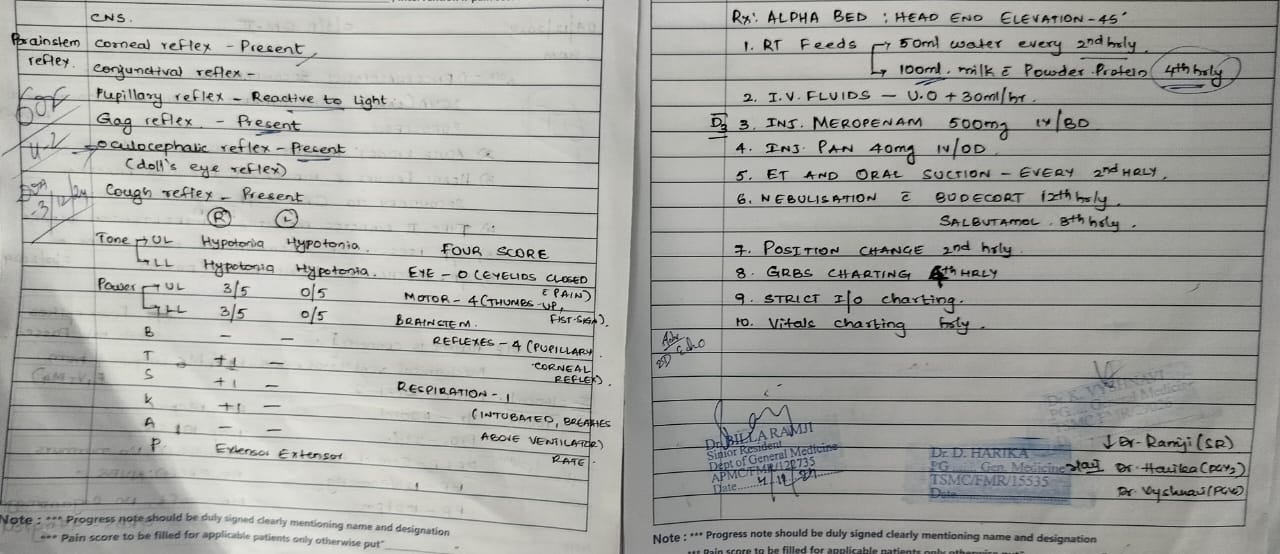
PPM 1 - Clinical findings by @PPM5.
PPM 2 -
Brilliant work and I'm being serious every IM trainee here would dream of wanting to do such clinical work.
What a topsy turvy world this is. The first worlders are doing social health and occupational therapy referrals while the third world has the brains but no resources!
@PPM6.
PPM 1 - 👍
PPM 6 - 👍
EMR Summary.
Age/Gender : 67 Years/Female
Address :
Discharge Type: Relieved
Admission Date: 03/12/2024 04:47 PM
Discharge Date
Date: Ward: Unit:
Name of Treating
Investigations
Name Value Name Value
RFT 03-12-2024 05:45:PM LIVER FUNCTION TEST (LFT) 03-12-2024 05:45:PM
UREA 106 mg/dl Total Bilurubin 2.44 mg/dl
CREATININE 4.2 mg/dl Direct Bilurubin 0.25 mg/dl
URIC ACID 4.4 mmol/L SGOT(AST) 36 IU/L
CALCIUM 8.6 mg/dl SGPT(ALT) 13 IU/L
PHOSPHOROUS 4.89 mg/dl ALKALINE PHOSPHATASE 133 IU/L
SODIUM 131 mmol/L TOTAL PROTEINS 4.9 gm/dl
POTASSIUM 4.1 mmol/L. ALBUMIN 2.23 gm/dl
CHLORIDE 101 mmol/L A/G RATIO 0.84
HBsAg-RAPID 03-12-2024 05:45:PM Negative Anti HCV Antibodies - RAPID 03-12-2024 05:45:PM Non Reactive
COMPLETE URINE EXAMINATION (CUE) 03-12-2024 05:45:PM ABG 04-12-2024 12:14:AM
COLOUR Pale yellow PH 7.40
APPEARANCE Clear PCO2 29.6
REACTION Acidic PO2 92.6
SP.GRAVITY 1.010 HCO3 17.9
ALBUMIN +++ St.HCO3 19.7
SUGAR Nil BEB -5.7
BILE SALTS Nil BEecf -6.0
BILE PIGMENTS Nil TCO2 38.1
PUS CELLS 4-5 O2 Sat 96.8
EPITHELIAL CELLS 2-3 O2 Count 11.4
RED BLOOD CELLS 4-5
CRYSTALS Nil
CASTS Nil
AMORPHOUS DEPOSITS Absent
OTHERS Nil
RFT 04-12-2024 03:58:AM ABG 04-12-2024 03:59:AM
UREA 129 mg/dl PH 7.39
CREATININE 4.6 mg/dl PCO2 20.9
URIC ACID 5.0 mmol/L PO2 106
CALCIUM 9.2 mg/dl HCO3 12.6
PHOSPHOROUS 6.0 mg/dl St.HCO3 15.3
SODIUM 134 mmol/L BEB -11.2
POTASSIUM 4.1 mmol/L. BEecf -11.3
CHLORIDE 99 mmol/L TCO2 27.9
O2 Sat 97.7
O2 Count 7.5
ABG 04-12-2024 04:42:PM ABG 05-12-2024 01:08:AM
PH 7.38 PH 7.37
PCO2 21.4 PCO2 21.7
PO2 107 PO2 104
HCO3 12.5 HCO3 12.5
St.HCO3 15.4 St.HCO3 16.1
BEB -11.3 BEB -10.7
BEecf -11.7 BEecf -11.7
TCO2 26.9 TCO2 24.9
O2 Sat 97.6 O2 Sat 97.1
O2 Count 10.2 O2 Count 18.1
RFT 05-12-2024 01:08:AM ABG 05-12-2024 08:01:PM
UREA 85 mg/dl PH 7.42
CREATININE 2.8 mg/dl PCO2 26.8
URIC ACID 3.0 mmol/L PO2 169
CALCIUM 9.4 mg/dl HCO3 17.1
PHOSPHOROUS 4.1 mg/dl St.HCO3 19.7
SODIUM 139 mmol/L BEB -5.8
POTASSIUM 4.0 mmol/L. BEecf -6.5
CHLORIDE 104 mmol/L TCO2 35.1
O2 Sat 98.8
O2 Count 15.0
LIVER FUNCTION TEST (LFT) 05-12-2024 11:43:PM RFT 05-12-2024 11:43:PM
Total Bilurubin 0.56 mg/dl UREA 147 mg/dl
Direct Bilurubin 0.16 mg/dl CREATININE 3.8 mg/dl
SGOT(AST) 19 IU/L URIC ACID 4.5 mmol/L
SGPT(ALT) 17 IU/L CALCIUM 9.8 mg/dl
ALKALINE PHOSPHATASE 178 IU/L PHOSPHOROUS 4.1 mg/dl
TOTAL PROTEINS 5.0 gm/dl SODIUM 138 mmol/L
ALBUMIN 2.01 gm/dl POTASSIUM 4.2 mmol/L.
A/G RATIO 0.67 CHLORIDE 101 mmol/L
ABG 05-12-2024 11:44:PM ABG 06-12-2024 10:02:PM
PH 7.40 PH 7.43
PCO2 28.8 PCO2 29.4
PO2 100 PO2 111
HCO3 17.7 HCO3 19.2
St.HCO3 20.0 St.HCO3 21.2
BEB -5.4 BEB -3.8
BEecf -6.1 BEecf -4.3
TCO2 36.0 TCO2 39.8
O2 Sat 97.2 O2 Sat 98.1
O2 Count 16.0 O2 Count 13.5
ABG 06-12-2024 11:51:PM RFT 06-12-2024 11:51:PM
PH 7.41 UREA 112 mg/dl
PCO2 27.6 CREATININE 2.5 mg/dl
PO2 120 URIC ACID 2.6 mmol/L
HCO3 17.4 CALCIUM 9.1 mg/dl
St.HCO3 19.5 PHOSPHOROUS 4.1 mg/dl
BEB -6.0 SODIUM 132 mmol/L
BEecf -6.3 POTASSIUM 4.4 mmol/L.
TCO2 37.1 CHLORIDE 99 mmol/L
O2 Sat 98.3
O2 Count 10.8
ABG 07-12-2024 10:11:PM RFT 07-12-2024 10:11:PM
PH 7.45 UREA 86 mg/dl
PCO2 28.3 CREATININE 1.9 mg/dl
PO2 90.5 URIC ACID 2.2 mmol/L
HCO3 19.7 CALCIUM 9.8 mg/dl
St.HCO3 21.5 PHOSPHOROUS 3.5 mg/dl
BEB -3.4 SODIUM 136 mmol/L
BEecf -3.6 POTASSIUM 3.7 mmol/L.
TCO2 42.7 CHLORIDE 99 mmol/L
O2 Sat 96.8
O2 Count 8.2
ABG 08-12-2024 05:44:PM ABG 08-12-2024 10:18:PM
PH 7.45 PH 7.500
PCO2 28.0 PCO2 26.3
PO2 77.7 PO2 111
HCO3 19.2 HCO3 20.3
St.HCO3 21.2 St.HCO3 22.7
BEB -3.8 BEB -2.0
BEecf -4.0 BEecf -2.4
TCO2 41.5 TCO2 43.1
O2 Sat 95.4 O2 Sat 98.2
O2 Count 8.9 O2 Count 10.2
LIVER FUNCTION TEST (LFT) 08-12-2024 10:19:PM RFT 08-12-2024 10:19:PM
Total Bilurubin 1.24 mg/dl UREA 60 mg/dl
Direct Bilurubin 0.26 mg/dl CREATININE 1.6 mg/dl
SGOT(AST) 16 IU/L URIC ACID 2.0 mmol/L
SGPT(ALT) 10 IU/L CALCIUM 8.8 mg/dl
ALKALINE PHOSPHATASE 224 IU/L PHOSPHOROUS 2.8 mg/dl
TOTAL PROTEINS 5.3 gm/dl SODIUM 134 mmol/L
ALBUMIN 2.02 gm/dl POTASSIUM 3.5 mmol/L.
A/G RATIO 0.62 CHLORIDE 98 mmol/L
ABG 09-12-2024 06:26:PM COMPLETE URINE EXAMINATION (CUE) 09-12-2024 08:00:PM
PH 7.45 COLOUR Pale yellow
PCO2 34.3 APPEARANCE Clear
PO2 79.5 REACTION Acidic
HCO3 24.0 SP.GRAVITY 1.010
St.HCO3 25.0 ALBUMIN +
BEB 0.7 SUGAR Nil
BEecf 0.5 BILE SALTS Nil
TCO2 51.2 BILE PIGMENTS Nil
O2 Sat 95.8 PUS CELLS 3-4
O2 Count 9.9 EPITHELIAL CELLS 2-3
RED BLOOD CELLS Nil
CRYSTALS Nil
CASTS Nil
AMORPHOUS DEPOSITS Absent
OTHERS Nil
RFT 09-12-2024 11:52:PM ABG 09-12-2024 11:53:PM
UREA 97 mg/dl PH 7.41
UREA 97 mg/dl PCO2 33.4
CREATININE 2.6 mg/dl PO2 65.3
CREATININE 2.6 mg/dl HCO3 21.0
URIC ACID 2.9 mmol/L St.HCO3 22.1
URIC ACID 2.9 mmol/L BEB -2.6
CALCIUM 9.1 mg/dl BEecf -2.8
CALCIUM 9.1 mg/dl TCO2 44.6
PHOSPHOROUS 3.8 mg/dl O2 Sat 92.1
PHOSPHOROUS 3.8 mg/dl O2 Count 10.6
SODIUM 134 mmol/L
SODIUM 134 mmol/L
POTASSIUM 3.6 mmol/L.
POTASSIUM 3.6 mmol/L.
CHLORIDE 92 mmol/L
CHLORIDE 92 mmol/L
ABG 10-12-2024 09:26:AM ABG 10-12-2024 12:03:PM
PH 7.43 PH 7.42
PCO2 35.2 PCO2 33.3
PO2 296 PO2 160
HCO3 23.3 HCO3 21.5
St.HCO3 24.4 St.HCO3 22.7
BEB -0.1 BEB -2.0
BEecf -0.4 BEecf -2.2
TCO2 47.3 TCO2 46.3
O2 Sat 99.4 O2 Sat 98.8
O2 Count 16.3 O2 Count 10.3
ABG 10-12-2024 05:08:PM RFT 10-12-2024 11:39:PM
PH 7.36 UREA 59 mg/dl
PCO2 43.5 CREATININE 1.6 mg/dl
PO2 184 URIC ACID 2.7 mmol/L
HCO3 23.9 CALCIUM 9.0 mg/dl
St.HCO3 23.7 PHOSPHOROUS 3.6 mg/dl
BEB -0.9 SODIUM 131 mmol/L
BEecf -0.8 POTASSIUM 3.7 mmol/L.
TCO2 52.1 CHLORIDE 93 mmol/L
O2 Sat 98.9
O2 Count 10.2
ABG 10-12-2024 11:40:PM RFT 11-12-2024 10:15:PM
PH 7.391 UREA 89 mg/dl
PCO2 37.5 CREATININE 2.7 mg/dl
PO2 128 URIC ACID 2.9 mmol/L
HCO3 22.2 CALCIUM 9.4 mg/dl
St.HCO3 22.8 PHOSPHOROUS 3.7 mg/dl
BEB -1.9 SODIUM 134 mmol/L
BEecf -2.0 POTASSIUM 3.6 mmol/L.
TCO2 47.4 CHLORIDE 96 mmol/L
O2 Sat 98.3
O2 Count 11.7
When to Obtain Urgent Care
IN CASE OF ANY EMERGENCY IMMEDIATELY CONTACT YOUR CONSULTANT DOCTOR OR ATTEND EMERGENCY DEPARTMENT.
Preventive Care
AVOID SELF MEDICATION WITHOUT DOCTORS ADVICE,DONOT MISS MEDICATIONS. In case
of Emergency or to speak to your treating FACULTY or For Appointments, Please Contact: For Treatment Enquiries Patient/Attendent Declaration : - The medicines prescribed and the advice regarding preventive aspects of care ,when and how to obtain urgent care have been explained to me in my own language SIGNATURE OF PATIENT /ATTENDER SIGNATURE OF PG/INTERNEE SIGNATURE OF ADMINISTRATOR SIGNATURE OF FACULTY.
PPM 1 -


EMR SUMMARY
Age/Gender : 67 Years/Female
Address :
Discharge Type: Relieved
Admission Date: 14/12/2024 11:55 AM
Name of Treating
Diagnosis
CVA WITH LEFT HEMIPARESIS (AIS:LARGE INFARCT IN RIGHT HEMISPHERE OF BRAIN) HFREF SECONDARY TO OLD CAD
ASPIRATION PNEUMONIA(RESOLVED) ACUTE KIDNEY INJURY ON CKD
SEPSIS SEC TO GRADE 3 BED SORE IN B/L GLUTEAL REGION K/C/O HTN,DM SINCE 10 YEARS
CAD S/P PTCA IN 2023
S/P 2 SESSION HEMODIALYSIS
https://pajrcasereporter.blogspot.com/2024/12/67f-with-striking-cerebral-ptosis.html?m=1
Case History and Clinical Findings
CHIEF COMPLAINT: 67 YEAR OLD FEMALE WAS BROUGHT TO THE CASUALTY WITH C/O SNORING SINCE LAST NIGHT
HOPI: PATIENT WAS APPARENTLY ASYMPTOMATIC UNTIL LAST NIGHT THEN HAD C/O DECREASED SENSORIUM AND SNORING.
C/O HEMATURIA SINCE 1 DAY
NO C/O INVOLUNTARY MOVEMENTS, DECREASED URINE OUTPUT, FEVER,COUGH, SOB,VOMITINGS,LOOSE STOOLS
H/O LEFT HEMIPARESIS WITH AKI WITH CKD ON DIALYSIS WITH UROSEPSIS ADMITTED IN GENERAL MEDICINE DEPARTMENT.
PATIENT WAS INTUBATED I/V/O LOW GCS AND TRANSFERRED TO EMD. EXTUBATED AND WAS DISCHARGED ON 12/12/24
PAST HISTORY
K/C/O HTN AND DM SINCE 10 YEARS K/C/O CAD S/P PTCA IN 2023 GENERAL EXAMINATION :
PATIENT IS C/C/C
NO PALLOR, ICTERUS, CYANOSIS, CLUBBING, LYMPHEDENOPATHY, EDEMA OF FEET PRESENT PITTING TYPE GRADE 3
BP: 120/70 MMHG PR: 114 BPM
RR: 22 CPM SPO2: 78% AT RA GRBS:372 MG/DL
SYSTEMIC EXAMINATION :
CVS: S1S2 + RS: BLAE +
B/L DIFFUSE COARSE CREPTS P/A: SOFT, NON TENDER
CNS: NO FND
SURGERY REFERRAL DONE I/V/O BEDSORE ON 14/12/24
ADVISED: FREQUENT POSITION CHANGE, ALPHA BED, REGULAR PRESURE DRESSING, DEBRIDEMENT REQUIRED AFTER STOPPING ANTICOAGULANTS FOR 5 DAYS , NEOSPOLIN POWDER FOR L/A
COURSE IN HOSPITAL
PT WAS ADMITTED IN VIEW OF ABOVE SAID COMPLAINTS AND WAS DIAGNOSED AS CVA WITH LEFT HEMIPARESIS (AIS:LARGE INFARCT IN RIGHT HEMISPHERE OF BRAIN) HFREF SECONDARY TO OLD CAD
ASPIRATION PNEUMONIA(RESOLVED) ACUTE KIDNEY INJURY ON CKD
SEPSIS SEC TO GRADE 3 BED SORE IN B/L GLUTEAL REGION K/C/O HTN,DM SINCE 10 YEARS
CAD S/P PTCA IN 2023
S/P 2 SESSION HEMODIALYSIS
PT WAS MANAGED WITH 2 SESSIONS OF HEMODIALYSIS ON 14TH AND 15/12/24, DIURETICS, IV ANTIBIOTICS, BETA BLOCKERS, ANTI PLATELETS, ANTI HYPERTENSIVES.
GENERAL SURGERY REFERRAL WAS TAKEN I/V/O BEDSORES AND ADVICE FOLLOWED. NEPHROLOGIST OPINION WAS TAKEN IN VIEW OF INCREASED UREA AND CREATININE, MEDICAL MANAGED WAS ADVICED AND ASKED TO REVIEW TO NEPHROLOGY OP AFTER 3
DAYS.
PT IS BEING DISCHARGED IN HEMODYNAMICALLY STABLE CONDITION.
Investigation
NameValueRangeNameValueRangeABG 14-12-2024 12:34:PM PH7.34PCO225.2PO280.4HCO313.5St.HCO315.7BEB-10.8BEecf-11.1TCO229.2O2 Sat94.2O2
Count9.9HBsAg-RAPID14-12-2024 12:34:PMNegative Anti HCV Antibodies - RAPID14-12-2024 12:34:PMNon Reactive RFT 14-12-2024 12:35:PM UREA146 mg/dl50-17 mg/dlCREATININE3.5
mg/dl1.2-0.6 mg/dlURIC ACID6.5 mmol/L6-2.6 mmol/LCALCIUM9.5 mg/dl10.2-8.6 mg/dlPHOSPHOROUS6.3 mg/dl4.5-2.5 mg/dlSODIUM136 mmol/L145-136 mmol/LPOTASSIUM4.5 mmol/L.5.1-3.5 mmol/L.CHLORIDE92 mmol/L98-107 mmol/LLIVER FUNCTION TEST (LFT) 14-12-
2024 12:35:PM Total Bilurubin1.20 mg/dl1-0 mg/dlDirect Bilurubin0.18 mg/dl0.2-0.0 mg/dlSGOT(AST)33 IU/L31-0 IU/LSGPT(ALT)15 IU/L34-0 IU/LALKALINE PHOSPHATASE189 IU/L141-53 IU/LTOTAL PROTEINS5.8 gm/dl8.3-6.4 gm/dlALBUMIN2.4 gm/dl4.6-3.2 gm/dlA/G RATIO0.71RFT 15-12-2024 12:04:AM UREA105 mg/dl50-17 mg/dlCREATININE2.6 mg/dl1.2-0.6
mg/dlURIC ACID4.4 mmol/L6-2.6 mmol/LCALCIUM9.7 mg/dl10.2-8.6 mg/dlPHOSPHOROUS3.9 mg/dl4.5-2.5 mg/dlSODIUM135 mmol/L145-136 mmol/LPOTASSIUM3.9 mmol/L.5.1-3.5 mmol/L.CHLORIDE96 mmol/L98-107 mmol/LSERUM CREATININE15-12-2024 05:03:PM2.8
mg/dl1.2-0.6 mg/dlRFT 15-12-2024 11:42:PM UREA77 mg/dl50-17 mg/dlCREATININE1.9 mg/dl1.2-
0.6 mg/dlURIC ACID2.9 mmol/L6-2.6 mmol/LCALCIUM9.6 mg/dl10.2-8.6 mg/dlPHOSPHOROUS3.1 mg/dl4.5-2.5 mg/dlSODIUM135 mmol/L145-136 mmol/LPOTASSIUM3.7 mmol/L.5.1-3.5 mmol/L.CHLORIDE98 mmol/L98-107 mmol/L
HAEMOGLOBIN 8.7 gm/dl TOTAL COUNT 21,600 cells/cumm NEUTROPHILS 90 % LYMPHOCYTES 06 % EOSINOPHILS 00 % MONOCYTES 04 % BASOPHILS 00 % PCV 25.0 vol % M C V 80.9 fl M C H 28.1 pg M C H C 34.7 % RDW-CV 15.2 % RDW-SD 47.2 fl RBC COUNT 3.09
millions/cumm PLATELET COUNT 3.98 lakhs/cu.mm SMEAR
RBC Normocytic normochromic
WBC Increased on smear with IncreasedneutrophilsPLATELETS Adeqaute HEMOPARASITES No hemoparasites seen IMPRESSION Normocytic normochromic anemiawith neutrophilic leucocytosis
RFT
UREA 185 mg/dl CREATININE 5.0 mg/dl URIC ACID 7.3 mmol/L CALCIUM 9.6 mg/dl
PHOSPHOROUS 7.3 mg/dl SODIUM 136 mmol/L POTASSIUM 5.7 mmol/L. CHLORIDE 98 mmol/L
HEMOGRAM 23-12-24
HAEMOGLOBIN 8.4gm/dl TOTAL COUNT 15,400 cells/cumm NEUTROPHILS 88 % LYMPHOCYTES 06 % EOSINOPHILS 00 % MONOCYTES 05% BASOPHILS 00 % PCV 24.5 vol % M C V 80.4 fl M C H 27.6 pg M C H C 34.3 % RDW-CV 15.8 % RDW-SD 49.1 fl RBC COUNT 3.05
millions/cumm PLATELET COUNT 3.13 lakhs/cu.mm SMEAR
RBC Normocytic normochromic
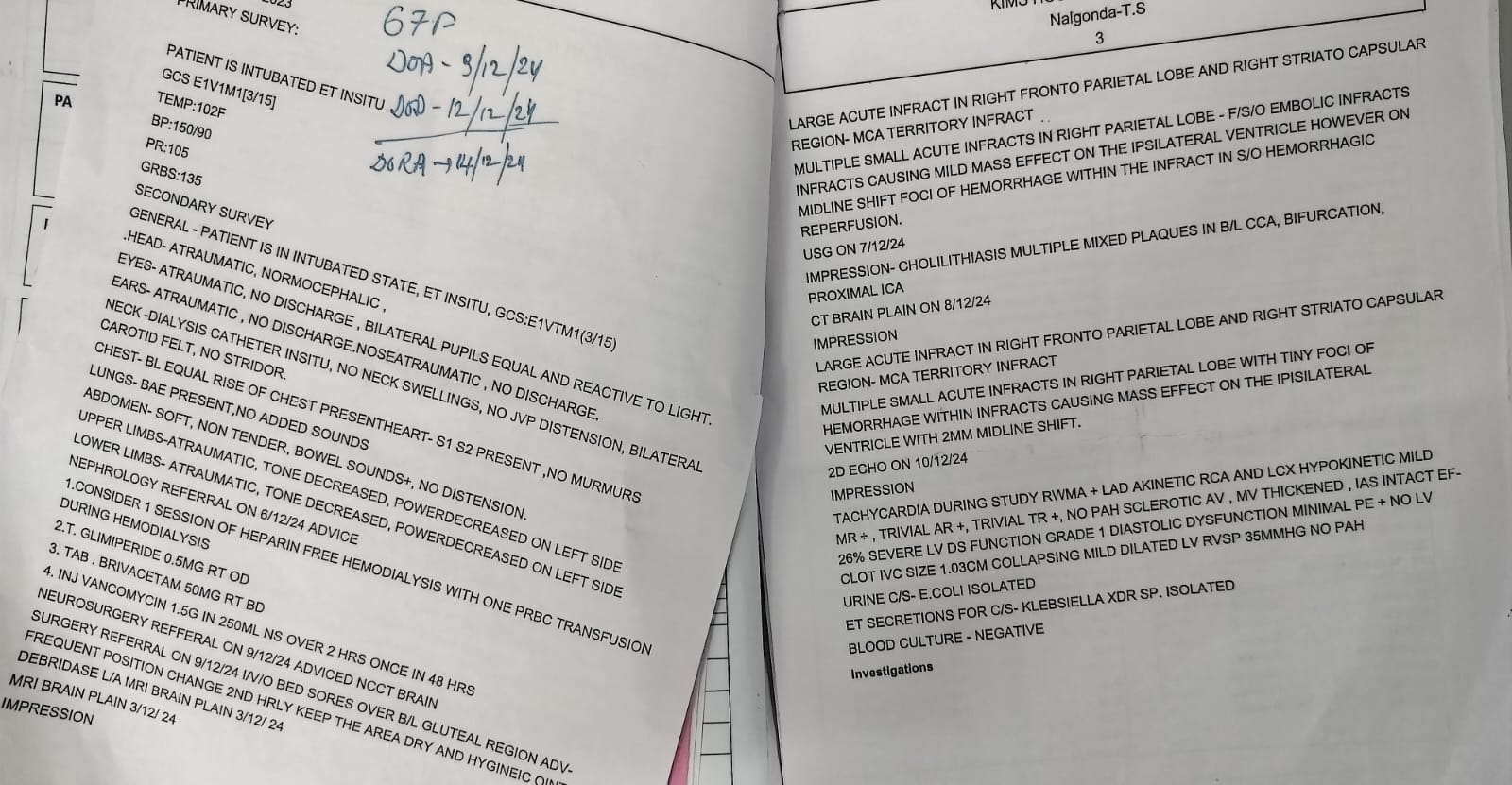
USG: RIGHT GRADE I RPD CHANGES GB SLUDGE WITH CALCULI
INCREASED ECHOGENICITY OF LEFT KIDNEY 2D ECHO:
TACHY CARDIA DURING STEADY
GLOBAL HYPOKINETIC, MODERATE TO SEVERE MR + MILD AR+ MODERATE TR+ MILD PAH, TRIVIAL TR+ SCLEROTIC AV, MV THICKENED,NO AS/MS
EF 28%, SEVERE LV Dysfunction PRESENT
DIASTOLIC DYSFUNCTION +, IVC MILD DILATED NON COLLAPSING ALL CHAMBERS DILATED
Treatment Given(Enter only Generic Name)
ALLOW SOFT DIET
INJ MEROPENEM 500MG IN 100ML NS IV/BD INJ VANCOMYCIN IN 250ML NS IV/STAT TAB PAN 40MG PO/OD
INJ HAI SC TID A/C GRBS
T. METXL 25MG PO/BD
T. ECOSPIRIN AV 75/20 RT/HS
T. DYTOR 20 MG PO/BD
T. DIGOXIN 0.35MG PO@ 8 AM ON FRIDAY, SATURDAY NEB WITH BUDECORT DUOCIN 8TH HRLY
2ND HRLY POSITION CHANGE HEAD END ELEVATION
GRBS PREMEAL MONITORING
INJ. SODIUM BICARBONATE 4 AMP IN 500 ML D5 IV/ STAT + LASIX 40 MG IV/ STAT+ INJ HAI 10 UNITS
TAB. TELMISARTAN 20 MG ONCE DAILY TAB. CINOD 10 MG ONCE DAILY BEDSORE DRESSING
16/12/24
HAEMOGLOBIN 8.7 gm/dl TOTAL COUNT 21,600 cells/cumm NEUTROPHILS 90 % LYMPHOCYTES 06 % EOSINOPHILS 00 % MONOCYTES 04 % BASOPHILS 00 % PCV 25.0 vol % M C V 80.9 fl M C H 28.1 pg M C H C 34.7 % RDW-CV 15.2 % RDW-SD 47.2 fl RBC COUNT 3.09
millions/cumm PLATELET COUNT 3.98 lakhs/cu.mm SMEAR
RBC Normocytic normochromic
WBC Increased on smear with Increased
neutrophils
PLATELETS Adequate HEMOPARASITES No hemoparasites seen IMPRESSION Normocytic normochromic anemia with neutrophilic leucocytosis
Advice at Discharge
TAB.LINEZOLID 600MG PO/BD FOR 10 DAYS
T. METXL 50MG PO/OD 1-0-0 TO BE CONTINUED
T. ECOSPIRIN AV 75/20 RT/HS 0-0-1 TO CONTINUE
T. DYTOR 40MG-0-20MG PO/BD TO CONTINUE (8AM)-0-(4PM)
T. DIGOXIN 0.25MG PO@ 8 AM ON FRIDAY, SATURDAY TAB. CINOD 10 MG PO/OD
TAB NODOSIS 500MG PO/BD 1-0-1 FOR 5 DAYS TAB SHELCAL CT PO/OD 0-1-0
INJ HAI SC/TID 4U-4U-6U
TAB PAN 40MG PO/OD/BBF 1-0-0 X 5 DAYS 2ND HRLY POSITION CHANGE
BEDSORE DRESSING
Follow Up
REVIEW AFTER 5 DAYS IN GM OPD/SOS
When to Obtain Urgent Care
IN CASE OF ANY EMERGENCY IMMEDIATELY CONTACT YOUR CONSULTANT DOCTOR OR ATTEND EMERGENCY DEPARTMENT.
Preventive Care
AVOID SELF MEDICATION WITHOUT DOCTORS ADVICE,DONOT MISS MEDICATIONS. In case
of Emergency or to speak to your treating FACULTY or For Appointments, Please Contact: For Treatment Enquiries Patient/Attendent Declaration : - The medicines prescribed and the advice regarding preventive aspects of care ,when and how to obtain urgent care have been explained to me in my own language
SIGNATURE OF PATIENT /ATTENDER
SIGNATURE OF PG/INTERNEE
SIGNATURE OF ADMINISTRATOR
SIGNATURE OF FACULTY
Discharge Date Date: 23/12/24 Ward:ICU
Unit:II
https://pajrcasereporter.blogspot.com/2024/12/67f-with-striking-cerebral-ptosis.html?m=1
No comments:
Post a Comment