
14-10-2024
This is an online E Log book to discuss our patient's de-identified health data shared after taking his signed informed consent. Here we discuss our patient's problems through series of inputs from available global online community experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.
In this case the patient is a 70yr old male admitted with sudden fever intermittent associated with chills and rigors.
Pyrexia of unknown origin heart failure with mid range ejection[EF 43%] B/L mild to moderate pleural effusion incisional hernia, sub acute intestinal obstruction.
K/C/O DM since 4 yrs.
HTN since 2 yrs.
CHIEF COMPLAINTS:
C/O fever since 1 week.
HISTORY OF PRESENT ILLNESS
Patient was apparently normal before 1 week. Suddenly developed fever intermittent associated with chills and rigors.
No H/O cough, cold, vomiting, diarrhoea, burning micturition.
HISTORY OF PAST ILLNESS
K/C/O T2 DM since 4 yrs on Tab.Metformin.
K/C/O HTN since 2 yrs on Tab.Telma 40mg
N/K/C/O TB, Asthma, Epilepsy, CAD, Thyroid Disorders.
GENERAL EXAMINATION
Patient is C/C/C. No Pallor, Icterus, Cyanosis, Clubbing, Lymphadenopathy, Edema.
BP - 110/70 might
PR - 98 B/M
RR - 18 CPM
Temperature - 100°F.
SYSTEMIC EXAMINATION
CVS - S1 S2+
RS - BAE + NVBS heard P/A inspection.
Shape - Scaphoid
Flanks - Free
Umbilicus - N inverted
Skin - N , Mild live scar present.
No dilated veins palpation diffuse tenderness present all over abdominal quadrants.
Liver and spleen- not palpable.
No Fluid thrill and shifting dullness.
No tidal percussion auscultation
Bowel sounds 20-30
Minnobruits CNS: No FND.
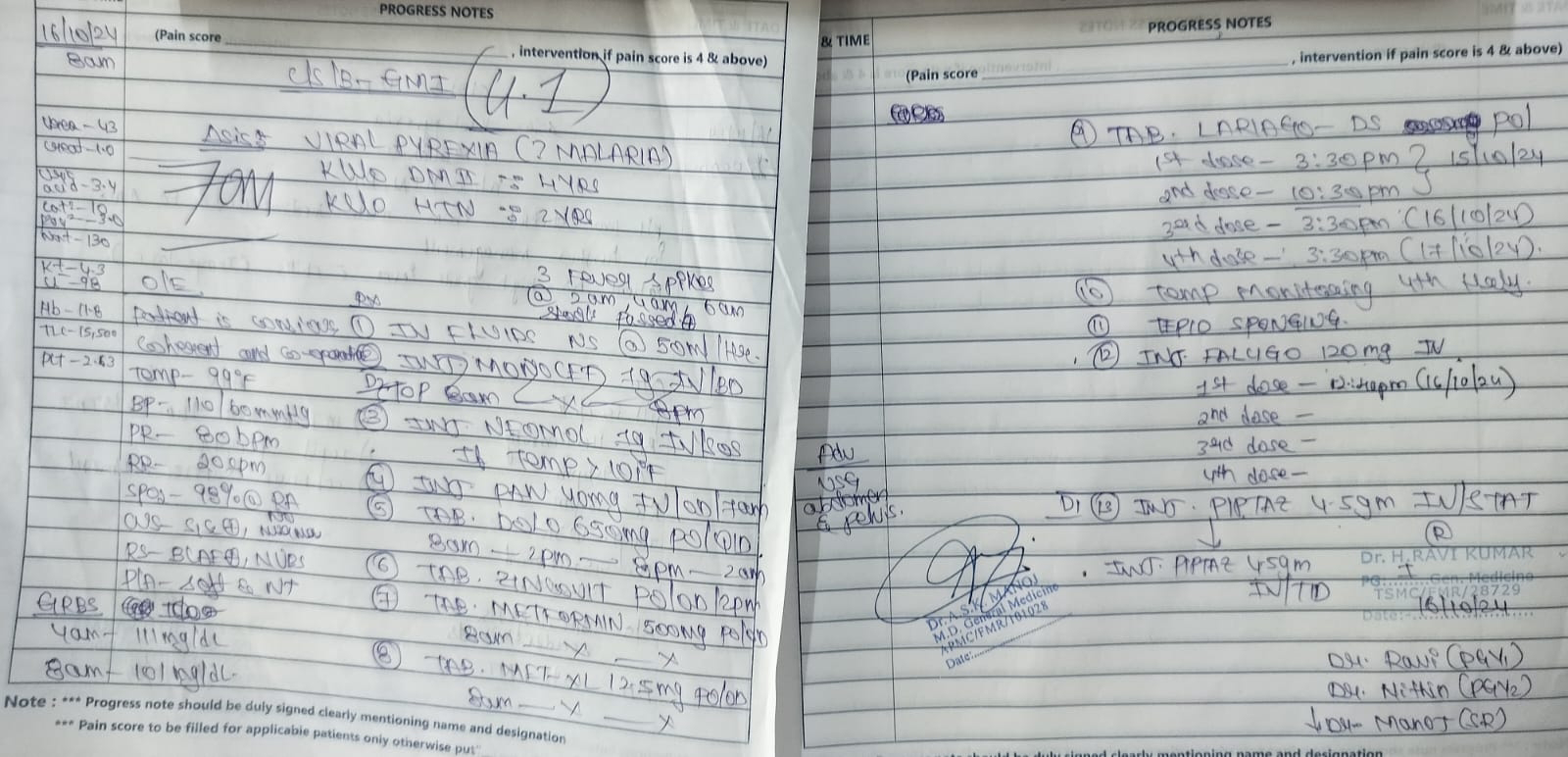
16-10-2024
PPM 1 - Admitted with fever since Monday and shifted to AMC today after fever didn't subside and now empirically started on treatment for Cefriaxone and Falcigo deficiency!
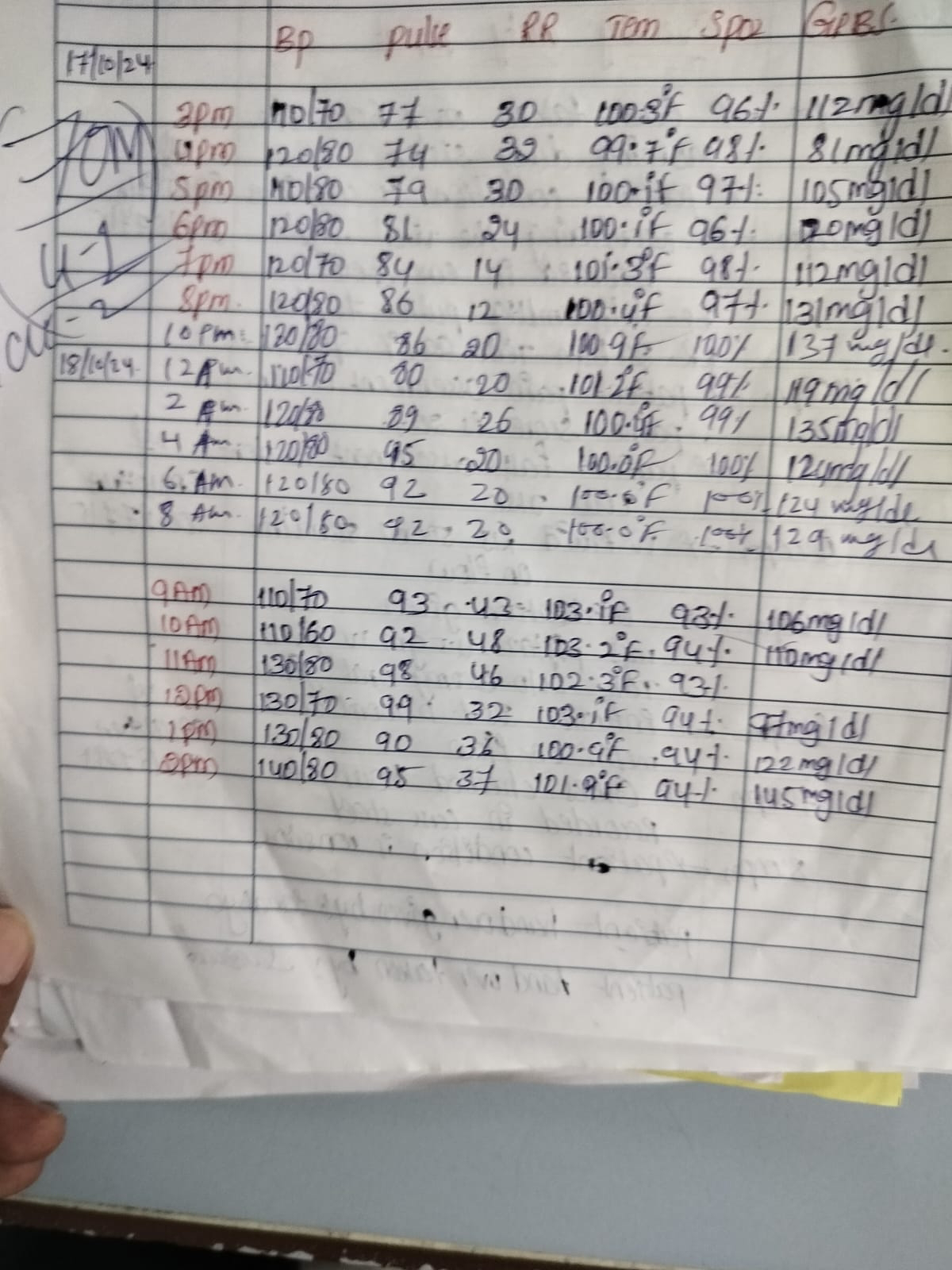
18-10-2024


PPM 1 - PUO shared earlier on antibiotic and antimalarial cocktail where this CT Abdomen may have detected something hiding behind it's ex laparotomy incision! Will try taking further data regarding the incision that was perhaps given long back and he just has a scar now. Unfortunately the fever data has begun to be captured 3 days after admission.
PPM 1 - 70M with PUO and a step ladder sepsis pattern @PPM2 indicative of a sepsis syndrome although it's currently still indifferentiated.

PPM 2 - Okay Sir.

PPM 1 - 70M ABG who has by now gone into severe tachypnoea with hourly serial respiratory rates of above 40/min @PPM2 which value of bicarbonate would you consider between the two shown here?@Metacognitist Mover &Shaker 1?
I remember you have taken a class on that. Can you share the link to the blog you had gathered the material from?
PPM 2 - Standard bicarb provides a direct handle on what the Metabolic system is doing, actual bicarb depends on PCO2 ie.taking into consideration the respiratory component also. (If the PCO2 is high, the HCO3 is dragged higher and vice versa).
https://pmc.ncbi.n/m.gov/articles/PMC5873626/.
So in this patient I would consider standard bicarb as his increased respiratory rate is probably because of his pain, not an actual respiratory problem(although yesterday's CT is suggestive that his lungs are also beginning to be involved).
PPM 1 - Can you share some of those Hrct images?
What's the standard bicarb value and actual bicarb value in this patient's ABG?
What does (P)c mean here?
PPM 2 - Standard bicarb in this patient is 19.2, actual is 15.2 sir. (P)c mean bicarbonate ions in plasma calculated by using Henderson Harsubach equation (using PCO2 and pH of plasma from ABG sample) correct me if I am wrong sir.
PAJR PHYSICIST - Is this a radio meter ABG?
PPM 1 - @PPM2 Can you ask our biomedical engineer the answer to this.
PPM 2 - Sure Sir.
Yes sir it is a radio meter ABG
PPM 1 - Rdiometer is the name of the company?
PPM 2 - Yes Sir.
https://www.radiometer.com/en/products/blood-gas-testing/abl800-flex-blood-gas-analyzer.
This machine to be precise sir.
PAJR PHYSICIST - Correct. ABG is a very sensitive test. Ideally, the blood from the arteries need to go into the ABG as soon as possible beside is best. Some folks actually used EDTA instead of Heparin. And most important of all the ABG system needs to be cleaned and calibrated daily. The pH electrode need be kept in buffer solution, the PO2 electrode membrane need some flushing with light proteolytic agents that clog the membrane ores and if badly clogged need to be changed. Was part of the team that designed the sensor module of IL GEM in the late seventies. So had a special interest in ABGs.
19-10-2024
PPM 1 - The patient appears to have had a brief respite in his fever today.

Does this fever appear to be malarial pattern? He has already received one course of falcigo. In empirical therapy of malaria once fever continues after the course of falcigo is over what should be the next step? @PPM3 & PPM4.
21-10-2024
METACOGNITIST MOVER AND SHAKER 1 - Appears more like a picket fence? Never really touches the baseline. Perhaps an element of Hectic fever(varying by 2.5F everyday). So run of the mill differentials - Pyogenic abscess, TB, Autoimmune fevers. Any brief history you could give us sir? Only if you have the time.
Brucella? Any relevant social history Endocarditis? Any dental issues/relevant personal and social history. Echo?
PPM 1 - In brief before I run to catch the bus , one dog and buffalo.

MMS 1 - Private Institution operating like Sarkari one!
PPM 1 - No Sarkari place offers an echocardiography machine as a try to their PGs.
MMS 1 - After 6 yrs of relentless fighting. The modus operandi is Sarkari though.
Also have we localised the sorce of Sepsis sir? Organ or organ system?
PPM 1 - No it's an indifferentiated fever. Short of a video need to contend with this tilling when our toy is back?

What happened to his 24 urinary protein and creatinine.

MMS 1 - Thanks a lot for sharing sir. If those? Calcification are old then he probably had RHD because nothing else can explain mitral valve Calcifications? If those are probable vegetations then infective Endocarditis is quite likely? Perhaps fundoscopy Janeway lesions and oiler nodes can give clues.
PPM 1 - The cardiomegaly sure suggests a Chronic heart failure. Wish I could do his echo myself or even see the video before I comment on the report. Not sure what they have written about the Mitral Valve.
MMS 1 - Mitralisation of left heart border and dilated RA here. With plenty of pulmonary congestion. MAC? Mitral Annular Calcification? What else would MAC mean anyway? Also the tech's skills have advanced so much that they have nicely calculated aortic valve pressures and Mitral regurg jet area! That's impressive work tbh.
PPM 1 - Agree! But she always knew how to do that I thought. To understand her MAC we'll need to ask her tomorrow what she meant and @PPM4 please send him tomorrow for a review echocardiography at the OPD echo room and call me from the OPD to review alongwith the tech.
PPM 4 - Okay Sir.
MMS 1 - Surely MAC has been used for quite a few years now and it is Mitral Annular Calcification. But yes definitely worth a review.
PPM 1 - Is that common?
MMS 1 - The use of the term or the incidence of it?
PPM 1 - Both.
MMS 1 - Yes to both.
https://www.jacc.org/doi/10-1016/j.jacc2022.06.009.
The main pathophysiological consequences of MAC are Mitral valve dysfunction (stenosis and /or regurgitation), atrial fibrillation (AF), stroke, infective Endocarditis and death.
In the context of an aging Population, clinicians are increasingly confronted by patients with Mitral valve dysfunction and accompanying MAC who may benefit from surgically transcatheter Intervention.
PPM 1 - So next question naturally would be what's the incidence of Mitral stenosis in patients with common MAC?
MMS 1 - I will leave that to your team. Thank you sir. 😅
PPM 1 - Our team is Meta AI. @ Meta AI Please share studies with valid references that throw more light on the incidence of mitral annular calcification with demographics and particularly on the incidence of functional mitral stenosis in patients with mitral annular calcification.
META AI - Mitral Annular Calcification (MAC) is a condition where Calcium deposits form on the mitral valve annulus, leading to functional mitral stenosis.
Studies have shown that MAC is more prevalent in older adults, with a significant increase in incidence after the age of 60 1.
In fact one study found that MAC accounted for 10% 30% and 60% of mitral
stenosis cases in patients aged 60-70, 70-80 and over 80 yrs respectively 1.
DEMOGRAPHICS AND INCIDENCE
•Age : MAC is more common in older adults with a prevalence of 6% in patients over 80 yrs 1.
•Sex : There is no significant difference in MAC prevalence between men and
women 1.
•Comorbidities : Patients with Chronic Kidney Disease, Diabetes, Hypertension and atherosclerosis are more likely to develop MAC 1[6] [7]
FUNCTIONAL MITRAL STENOSIS
•MAC can lead to functional mitral stenosis due to reduced leaflet mobility and diastolic annular dilation 1.
•The incidence of functional mitral stenosis in patients with MAC ranges from 0.2% to 2.5% 1 [3]
•A study found MAC produced Hemodynamically significant obstruction in 6% of patients with a mean age of 83 yrs [4].
ASSOCIATED RISKS
•MAC is associated with increased risk of stroke, atrial fibrillation and mortality 1.
•Calcium Thickness is a strong predictors risk for myocardial Infarction and vascular death 1.
These findings highlight the importance of monitoring MAC in older adults, especially those with underlying Comorbidities. Regular echocardiographic assessments can help identify MAC and functional mitral stenosis, allowing for timely Intervention and management 1.
PPM 1 - @Meta AI What is the incidence of infective Endocarditis (IE) in patients with MAC but without functional mitral stenosis is relatively low but still significant.
STUDIES AND FINDINGS
1. A Meta- analysis of 14 studies (2017) reported an overall IE incidence rate of 0.6% per patient-year in patients with MAC.
2. A cohort study of 1.034 patients with MAC (2018) found an IE incidence rate of 1.1% per patient-year.
3. Another study published in the journal of the American College of Cardiology (2019) reported an IE incidence rate of 0.8% per patient-year in patients with MAC without significant mitral stenosis.
RISK FACTORS
Patient with MAC are at increased risk of IE due to:
1. Calcium deposits creating a nidus for bacterial colonization.
2. Altered valve architecture.
3. Associated comorbidities (eg. Diabetes, Chronic Kidney Disease).
SPECIFIC RISK FACTORS FOR IE IN MAC
1. Thickness of Calcium deposits (>5mm).
2. Presence of mitral regurgitation.
3. History of fibrillation.
4. Age >75 yrs.
5. Male sex.
GUIDELINES AND RECOMMENDATIONS
The American Heart Association (AHA) and European Society of Cardiology (ESC) guidelines recommend:
1. Antibiotic prophylaxis for dental procedures in patients with MAC and high risk features.
2. Regular clinical and echocardiographic monitoring.
3. Aggressive management of comorbidities.
KEY REFERENCES:
1. Otto et.al (2017). Mitral Annular Calcification and risk of infective Endocarditis. Journal of the American College of Cardiology, 70(11)1331-1339.
2. Singh et.al (2018) Incidence and Predictorsof infective Endocarditis in patients with Mitral Annular Calcification. European Heart Journal 39(22), 2031-2038.
3. Nishimura et.al (2019). Mitral Annular Calcification and risk of infective Endocarditis:
A systematic review and Meta-analysis. Journal of Cardiology, 73(2), 151-158.
Please consult these references and current guidelines for more detailed information.
PPM 1 - @Meta AI update:
Once any patient has already received one course of falcigo (artemesin) as empirical therapy of malaria but once fever continues after the course of falcigo is over what should be the next step?
Please share your statements with valid references.
Meta AI:- If a patient continues to experience fever after completing a course of artemisin-based therapy (ACT) such as artesunate(not falcigo) the next steps are crucial for effective management.
WHO GUIDELINES(2021)
(1) Re-evaluate the diagnosis:
Consider other causes of fever such as Malaria treatment failure - co infections(eg bacterial, viral) - other febrile illnesses.
(2) Conduct a malaria parasite count(if not already done)
(3) Assess for Signs of severe malaria or complications.
RECOMMENDED ACTIONS
1. Repeat malaria testing(RDT or Microscopy) to confirm treatment failure or re infection.
2. Consider alternative malaria treatment regimens:- If initial treatment was ACT, switch to another ACT or an alternative regimen(eg.quinine + doxycyclin) - if treatment failure consider adding a partner drug(eg.Lumefantrine).
3. Investigate and treat potential co-infe tons.
TREATMENT FAILURE DEFINITION:
•Fever persistence or recurrence within 14-28 days after completing treatment.
•Parasite density>1000/uL on day 2 or 3 after treatment initiation
TREATMENT OPTIONS
1. Artemether-Lumefantrine (Coartem)
2. Artesunate - a modiaquine
3. Quinine - doxycyclin
4. Atovaquone - propranolol (Malaria).
REFERENCE
1. World Health Organization (2021)
Guidelines for Treatment of Malaria. (3rd Ed.)
2. Centres for Disease Control and Pre vention(2022) Malaria Treatment
3. National Institute of Allergy and Infection Diseases(2022)- Malaria Treatment.
IMPORTANT
• Consult local treatment guidelines and expert opinion.
• Consider referral to a specialized center if possible.
• Monitor patients closely for signs of severe malaria or complications.
Please note that "Falcigo" is not a recognised anti malarial medication.
Ensure accurate medication names and dosages are used.
16-10-2024
Surgery referral done. I/V/O incisional hernia. They advised USG Abdomen and X Ray erect Abdomen which shows no abnormality detected.
17-10-2024
Surgery referral done. I/V/O mild Edema in the Bowel wall with a possibility of strangulation in RT incisional hernia on reviews USG and advised it can manage medically with no active general Surgical Intervention.
19-10-2024
Surgery referral done and advised RFT.
20-10-2024
Surgery referral done and advised X-RAY, erect Abdomen shows no air Fluid levels.
21-10-2024
Surgery referral done and advised 3 sips of oral fluids F/O by liquid diet.
22-10-2024
Active mobilization Surgery referral done and advised ABG, liquid to soft diet.
23-10-2024
Active mobilization Surgery referral done and advised liquid to soft diet.
ACTIVE MOBILIZATION COURSE IN HOSPITAL
Patient came with complaints of fever and pain abdomen since 6 days and all necessary investigation were done and were normal.
Tab.PCM 650mg and Inj.Taximis was given and then changed to Inj.Piptaz to decrease counts and then he complained of Pain abdomen for which USG Abdomen was done which showed incisional hernia with momentum and Bowel as content for which Surgery referral was done on 16-10-2024. They advised X-Ray, erect abdomen which shows no abnormality then continuous fever was observed then shifted to AMC. Continuous fever spikes were seen. Then shifted to ICU. His pain abdomen did not subside for which review USG was done showed strangulation at right incisional hernia for which again Surgery referral done and advised X.ray. Erect Abdomen showed no abnormality plain CT Abdomen done shows possibly early or sub acute Bowel obstruction. HRCT done which shows consolidation in a epically segment RT lung lower lobe- ineffective etiology segmental at electiasis in the LT lung lower lobe and RT lung middle lobe B/L mild to moderate pleural effusion [LT>RT] mild diffused Edema of left chest wall with FOCI of air in the soft tissue enlarged left axillary lymph. Nodes Measuring 10 to 12mm as there is no improvement in continuous fever.
Tab.Azithromycin and Inj.Dexa is given. There is improvement in patient condition and then shifted to AMC and then to ward and then advised to discharge.
14-10-2024
Blood Urea - 48mg/dl
Serum Creatinine - 1.3mg/dl
Serum Electrolytes
Sodium - 133mmol/L
Potassium - 4.0mmol/L
Chloride - 96mmol/L
COMPLETE URINE EXAMINATION (CUE)
Colour - Pale yellow
Appearance - Clear
Reaction - Acidic
SP Gravity - 1.010
Albumin - ++
Sugar - Nil
Bile salts - Nil
Bile pigments - Nil
Pus cells - 5-6
Epithelial cells - 4-5
RBC - Nil
Casts - Nil
Amorphous deposits - Absent
Others - Nil.
RFT
Urea - 43mg/dl
Creatinine - 1.2mg/dl
Uric acid - 3.9mmol/L
Calcium - 10.2mg/dl
Phosphorus - 2.omg/dl
Sodium - 126mmol/L
Potassium - 4.0mmol/L
Chloride - 95mmol/L
LFT
Total bilurubin - 1.65mg/dl
Direct bilurubin - 0.22mg/dl
SGOT (AST) - 53 IU/L
SGPT (ALT) - 47 IU/L
Alkaline phosphatase - 349 IU/L
Total proteins - 6.5gm/dl
Albumin - 2.94gm/dl.
A/G Ratio - 0.83
COMPLETE URINE EXAMINATION (CUE)
Colour - Pale yellow
Appearance - Clear
Reaction - Acidic
SP Gravity - 1.010
Albumin - Trace
Sugar - Nil
Bile salts - Nil
Bile pigments - Nil
Pus cells - 3-4
Epithelial cells - 2-3
RBC - Nil
Crystals - Nil
Casts - Nil
Amorphous deposits - Absent
Others - Nil
URINE PROTEIN CREATININE RATIO
Spot Urine Protein - 9.5mg/dl
Spot Urine Creatinine - 46.8mg/dl
Ratio - 0.20
BLOOD SUGAR
FBS - 107mg/dl
15 -10-2024
Blood Form P Strip Test Result
Blood form P Strip Test - Negative (-ve)
Blood parasites (Malarial parasite) Test Result - Malaria parasite Negative (-ve)
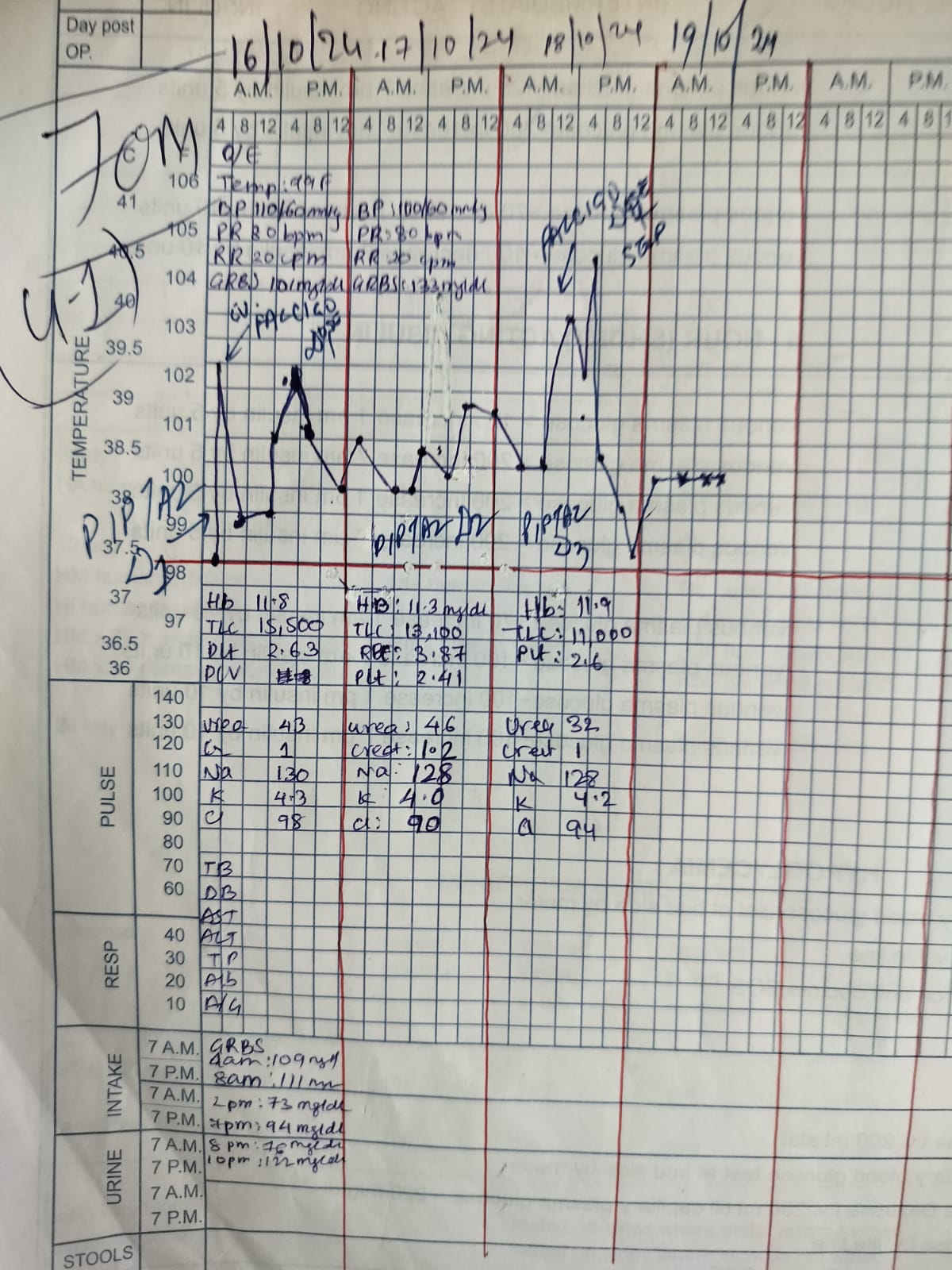
Hemoglobin - 11.8gm/dl
Total count - 15,500 cells/cumm
Neutrophils - 87%
Lymphocytes - 07%
Eosinophils - 00%
Platelet Count - 2.63 lakhs/cumm
Smear - Nomocytic Normochromic with Neutrophilic Leukocytosis
Urea - 43mg/dl
Creatinine - 1.0mh/dl
Uric acid - 3.4mmol/L
DHBS
Calcium - 10.0mg/dl
Phosphorus - 3.0mg/dl
Reduction Sodium - 130mmol/L
Electrode Potassium - 4.3mmol/L
Chloride - 98mmol/L
16-10-2024
COMPLETE URINE EXAMINATION
Colour - Pale yellow
Appearance - Clear
Reaction - Acidic
SP Gravity - 1.010
Albumin -+++
Sugar -Nil
Bile salts - Nil
Bile pigments - Nil
Pus cells - 3-4
Epithelial cells - 2-3
RBC - Nil
Crystals - Nil
Amorphous deposits - Absent
Others - Nil
USG IMPRESSION
Incisional hernia with Bowel and momentum herniation content B/L
Renal Cotical Cyst review.
17-10-2024
Hemoglobin - 11.3gm/dl
Total count - 13,100cells/cumm
Neutrophils - 92%
Basophils - 00%
Lymphocytes - 04%
Eosinophils - 01%
Monocytes - 03%
PCV - 32.2vol%
MCV - 83.2fl
MCH - 29.3pg
MCHC - 35.2%
RDW - CV - 14.0%
RDW - SD - 43.6fl.
RBC Count - 3.87 millions/cumm
Platelet Count - 2.41 lakhs/cumm
Smear RBC - Nomocytic Normochromic WBC- neutrophilic leukocytosis.
Platelets - Adequate
Haemoparasites - No Haemoparasites seen.
IMPRESSION
Normocytic Normochromic
17-10-2024
BLOOD PICTURE WITH NEUTROPHILIC LEUCOCYTOSIS
RFT
Urea - mg/dl
Creatinine - 1.2mg/dl
Uric acid - 2.1mmol/L
Calcium - 10.0mg/dl
Phosphorus - 2.7mg/dl
Sodium - 128mmol/L
17-10-2024
SEROLOGY NEGATIVE SERUM ELECTROLYTES TEST
Sodium - 130mmop/L
Potassium - 4.0mmol/L
Chloride - 94mmol/L
Calcium Ionized - 0.82mmol/L
HEMOGRAM
Hemoglobin - 11.9gm/dl
Total count - 11,000cells/cumm
Neutrophils - 85%
Lymphocytes - 11%
Eosinophils - 01%
Monocytes - 03%
Basophils - 00%
PCV - 32.7vol%
MCV - 82.0fl
MCH - 29.8pg
MCHC - 36.4%
RBW - CV - 14.0%
RBC Count - 3.99millions/cumm
Platelet Count - 2.06 lakhs/cumm
Smear RBC normocytic normochromic WBC with in normal limit.
Platelets - Adequate
Haemoparasites - No Haemoparasites seen.
IMPRESSION
Normocytic Normochromic blood picture with neutrophilic.
17-10-2024
Urea - 32mg/dl
Creatinine - 10mg/dl
Uric acid - 2.0mmol/L
Calcium - 10.0mg/dl
Phosphorus - 2.2mg/ dl
Sodium - 128mmol/L
Potassium - 4.2mmol/L
Chloride - 94mmol/L
USG DONE IE/O
Mild Edema in Bowel wall with possibility of strangulation over RT incisional hernia. No evidence of Bowel obstruction. 9 MM Supra umbilical hernia with momentum and Bowel as a herniation content CT Scan Abdomen plain done on 17-10-2024. Sub optimal evaluation due to motion artefacts, laxity in the anterior abdominal wall with super imposed Supra Umbilical defect Measuring 20mm with protrusion of small Bowel loop through the defects in the RT and LT para midline abdominal wall near umbilical region measuring 55mm and 20mm respectively with small volume herniation of multiple small Bowel loops few proximal Bowel loops are Mildly dilated with air Fluid levels possibly early or sub acute Bowel obstruction.
18-10-2024
ABG
PH - 7.45
PCO - 221.9mm
Hg PO - 239.3mmgh
HCO3 - 15.0mmol/L
St.HCO - 318.0mmol/L
BEB - 7.4mmol/L
BEecf - 8.2mmol/L
TCO2 - 31.3
Sat - 68.2%
Vol - 02
O2 count - 9.1vol%
BLOOD LACTATE TEST
Blood Lactate - 8.0mg/dl
COMPLETE URINE EXAMINATION (CUE)
Colour - Pale yellow
Appearance - Clear
Reaction - Acidic
SP Gravity - 1.010
Albumin - ++
Sugar - Nil
Bile salts - Nil
Bile pigments - Nil
Pus cells - 5-6
Epithelial cells - 2-3
RBC - 2-3
Crystals - Nil
Casts - Nil
Amorphous deposits - Absent
Others - Nil
ABG PH - 7.48
PCO2 - 20.5mmHg
PO2 - 65.7mmHg
HCO3 - 15.2mmol/L
St.HCO3 - 19.2mmol/L
BEB - 6.3mmol
BEecf - 7.7mmol/L
TCO2 - 30.1 vol o2
Sat - 92.7%
O2 count - 15.8vol%
18-10-2024
FERRITIN
KIMS Ferritin - 1270.7ng/ml
LIPASE
Serum Lipase - 34 IU/L
Serum Amylase - 4 IU/L
2D ECHO done.
Moderate TR with PAH, moderate MR mild arconcentric LVH, no RWMA, no MS, mild as good LV systolic function grade 1 diastolic function present.
19-10-2024
COMPLETE URINE EXAMINATION (CUE)
Colour - Pale yellow
Appearance - Clear
SP Gravity - 1.010
Reaction - Acidic
Albumin - +
Sugar - Nil
Bile salts - Nil
Bile pigments - Nil
Pus cells - 3-4
Epithelial cells - 2-3
RBC - Nil
Crystals - Nil
Casts - Nil
Amorphous deposits - Absent
Others - Nil
HEMOGRAM
Hemoglobin - 11.1gm/dl
Total count - 10,000 cells/cumm
Neutrophils - 80%
Lymphocytes - 14%
Eosinophils - 01%
Monocytes - 05%
Basophils - 00%
PCV - 29.8vol%
MCV - 79.9fl
MCH - 29.8pg
MCHC - 37.2%
RDW - CV - 13.8%
RDW - SD - 41.3fl
RBC Count - 3.73 millions/cumm
Platelet Count - 2.47 lakhs/cumm
Smear - RBC normocytic normochromic
WBC within normal limits.
Platelets - Adequate
Haemoparasites - Not Seen.
IMPRESSION
Normocytic normochromic blood picture.
19-10-2024
LFT
Total bilurubin - 1.37mg/dl
Direct bilurubin - 0.95mg/dl
SGOT (AST) - 68 IU/L
SGPT (ALT) - 44 IU/L
Alkaline phosphatase - 478 IU/L
Total proteins - 5.5gm/dl
Albumin - 2.0gm/dl
A/G Ratio - 0.59
Urea - 35mg/dl
Creatinine - 0.9mg/dl
Uric acid - 2.0mmol
Calcium - 10.0mg/dl
Phosphorus - 2.3mg/dl
Sodium - 132mmol/L
Potassium - 4.4mmol/L
Chloride - 99mmol/L
LFT
Total bilurubin - 1.4mg/dl
Direct bilurubin - 0.28mg/dl
SGOT (AST) - 73 IU/L
SGPT (ALT) - 43 IU/L
Alkaline phosphatase - 480 IU/L
Total proteins - 6.0gm/dl
Albumin - 2.0gm/dl
A/G Ratio - 0.51
Hemoglobin - 11.6gm/dl
Total count - 8,400 cells/cumm
Neutrophils - 83%
Eosinophils - 01%
Lymphocytes - 13%
Monocytes - 03%
Basophils - 00%
PCV - 31.3vol%
MCV - 80.3fl
MCH - 29.7pg
MCHC - 37.1%
RDW -CV - 14.1%
RDW -SD - 4.2fl
RBC Count - 3.9 millions/cumm
Platelet Count - 2.5 lakhs/cumm
Smear RBC - Normocytic normochromic WBC neutrophilic
Platelets - Adequate
Haemoparasites - Not seen
IMPRESSION
Normocytic normochromic blood picture with neutrophilic
19-10-2024
HEMOGRAM
Hemoglobin - 11.63gm/dl
Total count - 11,100 cells/cumm
Neutrophils - 82%
Eosinophils - 01%
Lymphocytes - 15%
Monocytes - 02%
Basophils - 00%
PCV - 30.9vol%
MCV - 8.9fl
MCH - 29.6pg
MCHC - 36.6%
RDW - CV - 14.5%
RDW - SD - 43.1fl
RBC 3 - 3.80 millions/cumm
Platelet Count - 2.6 lakhs/cumm
Smear - RBC normocytic normochromic WBC neutrophilia
Platelets - Adequate
Haemoparasites - Not seen
IMPRESSION
Normocytic normochromic blood picture with neutrophilia.
RFT
Urea - 35mg/dl
Creatinine - 0.9mg/dl
Uric acid - 2.0mmol/L
Calcium - 10.0mg/dl
Phosphorus - 2.3mg/dl
Sodium - 135mmol/L
Potassium - 4.3mmol/L
Chloride - 99mmol/L
20-10-2024
ABG
PH - 7.43
PCO2 - 24.3mmHg
PO2 - 69.9mmHg
HCO3 - 15.9mmol/L
St.HCO3 - 18.8mmol/L
BEB - 6.8mmol/L
BEecf - 7.6mmol/L
TCO2 - 32.6 vol o2
Sat - 93.2%
O2 count - 13.7vol%
HEMOGRAM
Hemoglobin - 11.3gm/
Total count - 11,100 cells/cumm
Neutrophils - 92%
Lymphocytes - 15%
Eosinophils - 01%
PCV - 30.9vol%
MCV - 80.9fl
MCH - 29.6pg
MCHC - 36.6%
RDW - CV - 14.5%
RDW -SD - 43.fl
RBC Count - 3.8 millions/cumm
Platelet Count - 2.6 lakhs/cumm
Smear - RBC normocytic normochromic WBC neutrophilic leucocytosis.
Platelets - Adequate
Haemoparasites - Not seen.
IMPRESSION - Normocytic normochromic with neutrophilic leucocytosis
RFT
Urea - 39mg/dl
Creatinine - 0.8mg/dl
Uric acid - 2.0mmol/L
Calcium - 10.0mg/dl
Phosphorus - 2.5mg/dl
Sodium - 130mmol/L
Potassium - 4.5mmol/L
Chloride - 102mmol/L
21-10-2024
HEMOGRAM
Hemoglobin - 11.7mg/dl
Total count - 6,900 cells/cumm
Neutrophils - 79%
Lymphocytes - 20%
Eosinophils - 00%
Monocytes - 01%
Basophils - 00%
PCV - 32.8vol%
MCV - 82.2fl
MCH - 29.3pg
MCHC - 35.7%
RDW - CV - 14.9%
RDW - SD - 45.0fl
RBC Count - 3.9 millions/cumm
Platelet Count - 2.4 lakhs/cumm
Smear - RBC normocytic normochromic WBC within normal limits.
Platelets - Adequate
Haemoparasites - Not seen.
RFT
Urea - 36mg/dl
Creatinine - 0.8mg/dl
Uric acid - 2.6mmol/L
Calcium - 10.2mg/dl
Phosphorus - 3.1mg/dl
Sodium - 132mmol/L
Potassium - 5.0mmol/L
Chloride - 104mmol/L
22-10-2024
PH - 7.37
PCO2 - 23.4mmHg
PO2 - 97.8mmHg
HCO3 - 13.4mmol/L
St.HCO3 - 16.3mmol/L
BEB - 10.2mmol/L
BEecf - 10.8mmol/L
TCO2 - 27.9 vol o2
Sat - 96.4%
O2 count - 13.7vol%
HS Troponin - 1 Test. Troponin - 142.8pg/nl
HRCT IMPRESSION
Consolidation in apical segment RT lung lower lobe- Ineffective etiology segmental at electiasis in the LT lung lower lobe and RT lung middle lobe. B/L mild to moderate pleural effusion [LT>RT].
Mild diffuse Edema of left chest wall with FOCI of air in the soft tissue enlarged left axillary lymph nodes measuring 10 to 12mm.
23-10-2024
Hemoglobin - 12.1gm/dl
Total count - 4,700 cells/cumm
Neutrophils - 70%
Lymphocytes - 23%
Eosinophils - 00%
Monocytes - 07%
Basophils - 00%
PCV - 34.2vol%
MCV - 82.4fl
MCH - 29.1pg
MCHC - 35.3%
RDW - CV - 14.6%
RDW - SD - 45.0fl
RBC Count - 4.15 millions/cumm
Platelet Count - 3.58 lakhs/cumm
Smear - RBC normocytic normochromic light Microscopy WBC with in normal limits.
Light Microscopy Platelets - Adequate in number and distribution.
Haemoparasites - Not seen
IMPRESSION
Normocytic normochromic blood picture.
RFT
Urea - 62mg/dl
Creatinine - 0.8mg/dl
Uric acid - 4.2mmol/L
Calcium - 10.0gm/dl
Phosphorus - 3.4mg/dl
Sodium - 132mmol/L
Potassium - 5.3mmol/L
Chloride - 101mmol/L
24-10-2024
Hemoglobin - 11.6gm/dl
Total count - 7,400 cells/cumm
Neutrophils - 67%
Lymphocytes - 23%
Eosinophils - 01%
Monocytes - 09%
Basophils - 00%
PCV - 33.1vol%
MCV - 83.5fl
MCH - 29.2pg
MCHC - 34.2%
RDW - CV - 14.4%
RDW - SD - 44.4fl
RBC Count - 3.9 millions/cumm
Platelet Count - 2.9 lakhs/cumm
Smear RBC - Normocytic normochromic WBC within normal limits.
Platelets - Adequate
Haemoparasites - Not seen.
IMPRESSION
Normocytic normochromic blood picture.
RFT
Urea - 71mg/dl
Creatinine - 0.8mg/dl
Uric acid - 3.4mmol/L
Calcium - 10.2mg/dl
Phosphorus - 2.6mg/dl
Sodium - 133mmol/L
Potassium - 4.7mmol/L
Chloride - 104mmol/L
MEDICATION
1. IV FNS at 50 ML/ HR
2. Tab.PCM 650mg PO/TID
3. Tab.MVT PO/OD
4. Tab.Pan 40mg PO/OD
5. Inj.Neomol IGM IVS TAT
6. Tab.Metformin 500mg PO/OD
7. Tab.Metexyl 12.5mg PO/OD
8. Tab.Larigodspo 1ST/2ND/3RD/4TH dose.
9. Inj.Placigo 120mg IV
10. Inj.Piptaz 4.5gm IV TID
11. Tab.Zincovit PO/OD
12. Inj.Ceffriaxone 1gm IVBD
13. Tab.Ecosprin AV 75/20 PO/OD
14. Tab.metxl 12.5mg OD
15. Tab.Metformin 500mg OD at 7am.
16. Tab.Dexamethasone 4mg PO/OD ×2 days.
Followed by Dexamethasone 2mg PO/OD × 2 days.
Followed by Dexamethasone 1mg PO/OD × 2 days
Review to GM OP SOS.
In case of any emergency immediately contact your consultant Doctor or attend emergency department.
No comments:
Post a Comment