
14-12-2024
This is an Online E Log Book to discuss our patient's de-identified health data shared after taking his signed informed consent. Here we discuss our patient's problems through series of inputs from available global online community experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.
PPM 1 - Reviewed the meningitis patient in the afternoon.
Comatose, Dolls eye sluggish with bilateral abducens palsy suggestive of a false localizing sign indicating raised ICT


Yesterday's afternoon and evening session:
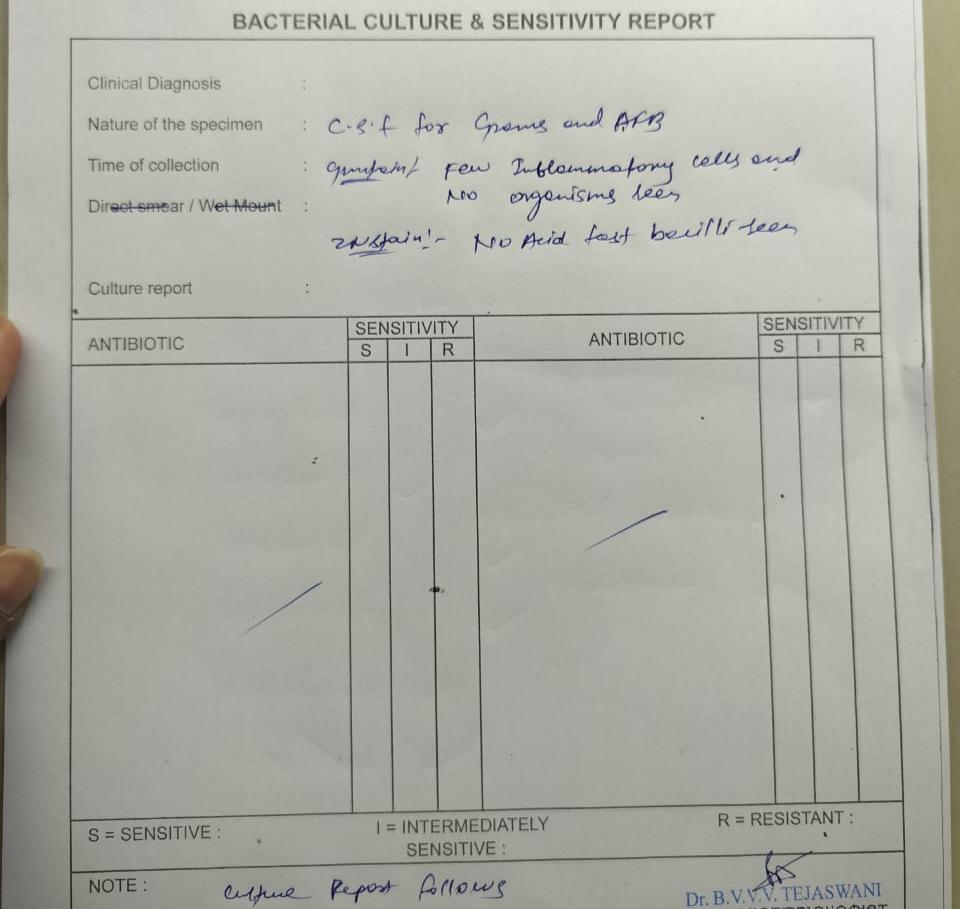
45M alcohol consumer 90-180 ml every day with severe headache and gradual development of altered sensorium over 4 days. When we saw her in the afternoon the psychiatry resident was asking the nurse to start him on iv lorazepam thinking of treating alcohol withdrawal when we stopped the nurse and convinced the psychiatry that this was more of an organic problem, which even they too had at the back of their minds and they readily agreed especially when we demonstrated mild positive meningeal signs and planned a CT head and lumbar puncture. The CSF showed high protein of 210 mg and CSF sugar 20 with corresponding blood sugar of 127 and WBC of 100 with 70 lymphos.
PPM 1 - High grade fever spikes continue. History reviewed and appears to have had low grade fever since one month beginning with the vesicular eruptions on his legs that turned into the ulcerations in the images shared above.
PPM 1 - 👆 @PPM3 Check out the K+ values and include him for your thesis project
@PPM4 please share the treatment order chart to demonstrate how we are tackling his hypokalemia and other issues.
PPM 3 - Yes sir Thank you.
17-12-2024
Update:
Was intubated and ventilated since 14/12/24
Still in altered sensorium
Tracheostomy done today.
18-12-2024
PPM 4 -

Repeat CSF done yesterday night
@PPM1 sir
Is it bacterial or viral ?
Responded to treatment?
PPM 1 - Thanks. I guess he also received iv acyclovir and either way one can say that microscopic the meningeal inflammation has reduced although you will need to tell us his clinical improvement.
Also share his fever chart.
PPM 4 - Okay sir
Will try to share
Sir we were not interested in starting Acyclovir
Was it a good decision to start acyclovir ?
Is it helpful in this case ?
PPM 1 - Good questions
Again in an individual patient without a parallel comparator it's always difficult to answer if the response was due to the intervention or was just due to time alone.
However you can review the literature if his clinical and CSF findings can be attributed to HSV encephalitis with reasonable certainty.
Do we have his MRI images?
PPM 4 - Only CT was done at admission sir
The EMD team repeated CT brain again yesterday
MRI was not done.
PPM 1 - Can you review the literature as to what would have been the best way to diagnose HSV encephalitis with reasonable certainty and if there are any trials around empirical therapy of HSV meningitis with acyclovir vs placebo?
PPM 4 - Sir also
We also thought of TB meningitis at once
Is it still the possibility
And we even started the pt on dexamethasone ,but it was stopped later on .Is it a good decision to stop ?
PPM 1 - So the next question is: Did the meningeal inflammation reduce due to the SAID?
The decision to stop any intervention depends on if the end objective of the intervention has been met, in this case if the inflammation subsided there wouldn't be much point in continuing the anti-inflammatory.
19-12-2024
PPM 4 -
There is no improvement in the patient’s condition sir
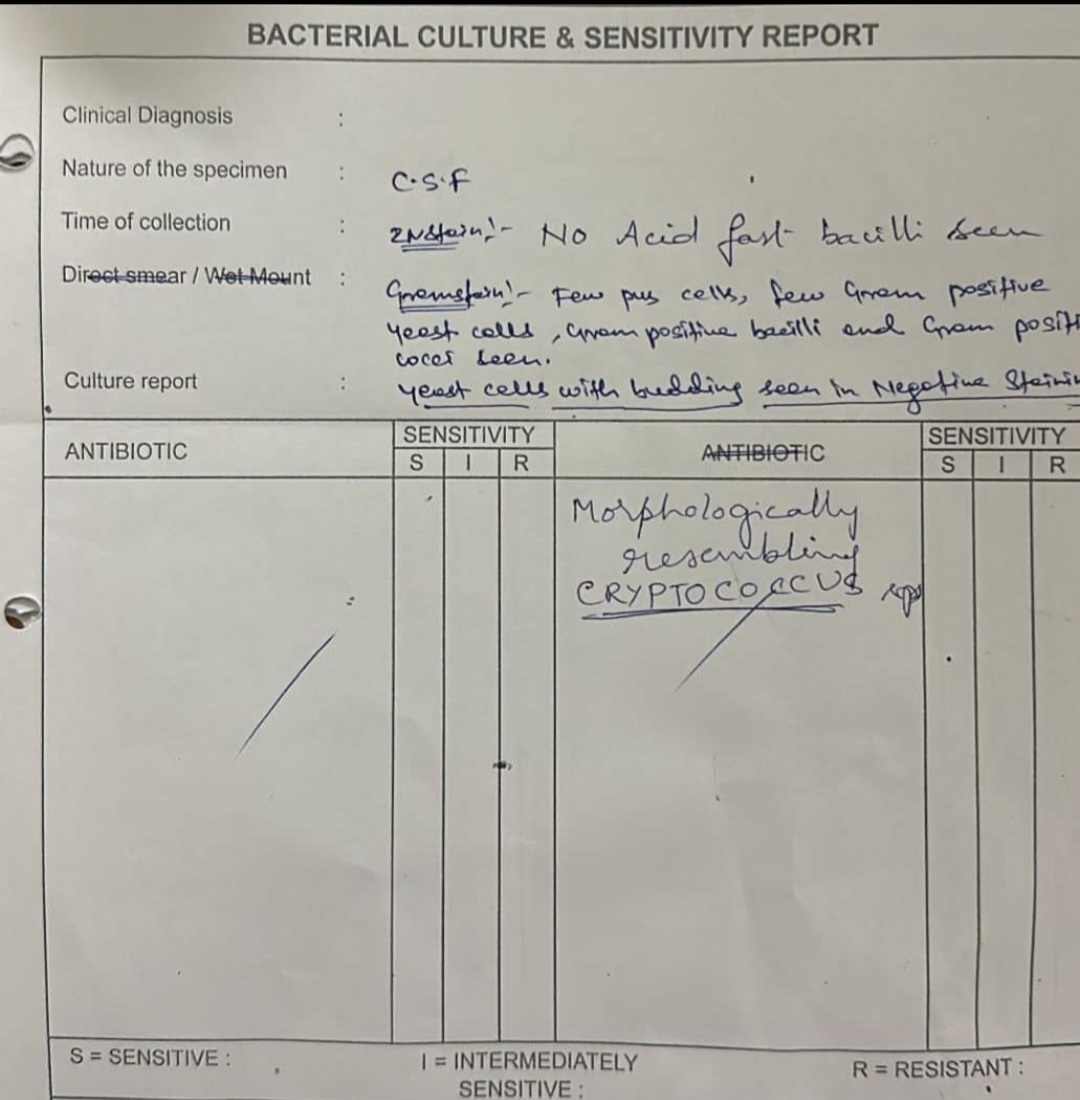
Repeat CSF done on 17/12/24 showed cryptococcus
Case has been referred today by EMD team
As per the micro team there was suscpicion of cryptococcus in the earlier sample too but they later denied its presence in the report as it might be a lymphocyte.
PPM 1 - 😮
Referred where? Government hospital? Please track what happens to him.
@PPM5 @PPM2 @PPM7 let's prepare an inventory of the many cryptococci and mucor we have isolated in the last few months.
PPM 4 - Ok sir
How come the micro team have missed it in first sample sir?
It might not be cryptococcus this time too?
Will try to share the image if possible.
PPM 4 - The sensitivity of India ink staining of CSF depends on fungal burden and is reported to be 30% to 50% in non–AIDS-related cryptococcal meningitis and up to 80% in AIDS-related disease. False positives can result from intact lymphocytes, other tissue cells and nonviable yeast forms, which further limits the diagnostic utility of direct microscopy of CSF for cryptococcal meningitis.
PPM 2 -
See if any study looks at how and why microscopic examination of Cryptococcus can be difficult?
This is a sensitivity study. What are the factors that led to low sensitivity?
PPM 4 -

PPM 8 - It's the same last week case??
PPM 9 - Yes sir.
PPM 8 - Share photos of his foot ulcers...PPM 10 - Patient is 40yr male ,Labourer by occupation who is chronic alcoholic & smoker(Non diabetic & Serology is negative)
What predisposed him for cryptococcus meningitis ??
The other clue we are having is ulcer over left foot(40days old) & sinus over right shin of tibia (10day old)
Is it a cutaneous cryptococcus dessimination ??
PPM 1 - 👍

Right

Left
PPM 7 -
Assuming his Chronic smoking can predispose him to PVD at microvascular level leading to non healing ulcer.
10 days is very acute to form a sinus tract.. is it osteomyelitis..? Any xray..?
Cryptococcus stained in CSF could entered CSF through hematogenous route.. if so PCR could be helpful to rule in dessiminated cryptococosis.
Any other pointers in history or examination favouring immunodeficiency ..?
PPM 1 -

👆Zoom view of the crypto.
PPM 8 - Patient is suspected to have psoriasis too..
This sort of ulcer appears to be a sign of immunodeficiency...
Hep B, Hep C, HIV sero status??
PPM 1 - 👍
PPM 8 - I'm convinced sir that cryptococcus is very likely in this patient...
PPM 1 - 👍
He died at his home today morning(19-12-2024) as gathered from our entire Telangana and Andhra Pradesh community network just by mentioning his village.
@PA please add this closure to his case report. Wish we had more data in his history events even before his cryptococcal events began to be able to get better insights into his overall life events.
PPM 1 - @PPM3 what were your thesis insights around his hypokalemia?
No comments:
Post a Comment