
This is an online E Log book to discuss our patient's de-identified health data shared after taking his signed informed consent. Here we discuss our patient's problems through series of inputs from available global online community experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.
To begin with a 65 Yr old male, resident of Chandur came with chief complaints of decreased urine volume, increased frequency of urination and poor stream
since 3 months.
HISTORY OF PRESENT ILLNESS.
Patient was apparently asymptomatic 3 months back and noticed decreased urine volume and poor stream which is not associated with pain, burning micturition, blood in urine, fever. Frequency of urination is increased.
PAST HISTORY
No similar complaints in the past.
He is a known case of diabetes since 20yrs with the below medication.
1. Sitagliptin 100mg
2. Metformin 500mg
3. Dapagliflozin 10mg
4. Injection Insulin isophane 48U-46U
5. Injection Insulin gargling 0U-16U.
Since 20yrs he is on the below medication for hypertension.
1. Olmesartan 20mg
2. Amlodipine 5mg
3. Hydrochlorthiazide 12.5mg.
Not a known case of Asthma, tuberculosis, epilepsy, CAD, CVD.
FAMILY HISTORY
Irrelevant
PERSONAL HISTORY
Diet - Mixed
Apetite- Normal
Bowel and bladder movements- Normal
Sleep- Inadequate
Addictions- No.
VITALS
Temperature- Afebrile
Pulse rate- 80bts/min
Respirate- 17cycles/min
BP- 124/82 might
GENERAL EXAMINATION
Patient's consent was taken. Patient was examined in a well lit room. He was conscious, coherent, cooperative. No Pallor, no Icterus, no Cyanosis, no Clubbing, no Lymphadenopathy. Pitting type of Pedal Edema is present.






Day 1
02-11-2023
8 am - 215
12pm - 289
4 pm - 341
6 pm- 356
10 pm - 327

he has taken.
STUDENT- OK Sir.
Day 2
03-11-2023
8 am - 143
12 pm - 274
4 pm - 344
6 pm - 304
10 pm - 340

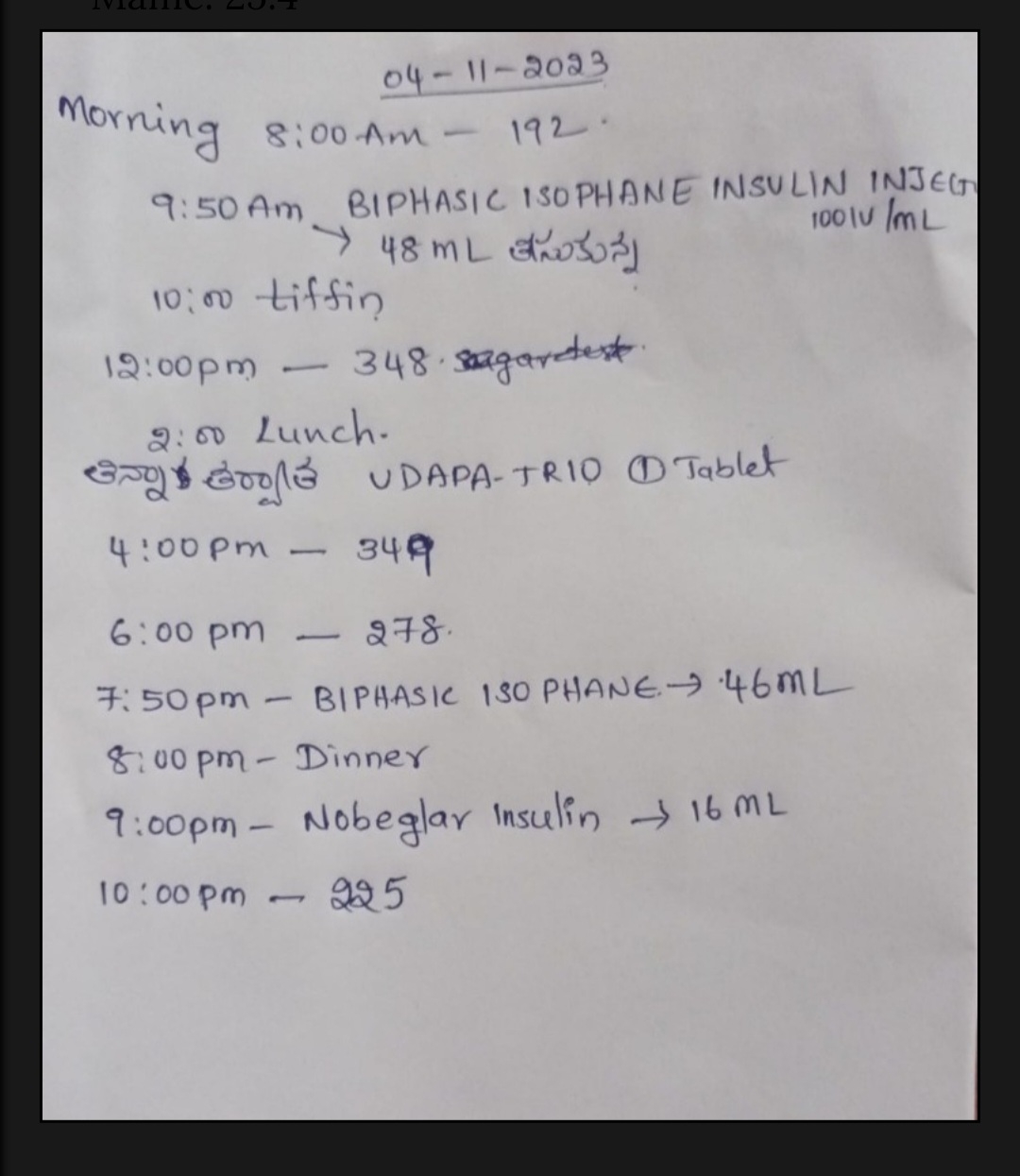
04-11-2023
8am - 192
12 pm - 348
4 pm - 349
6 pm - 278
10 pm - 225
05-11-2023
8 am - 99
12 pm - 278
4 pm - 327
6 pm - 320
10 pm - 183

PPM 1- Yes we need to optimize the dose .
First we need to separate the biphasic insulin into separate watery soluble Insulin and milky NPH Insulin. Just ask him to share the image of his current biphasic Insulin and you may find it's cloudy. But we also need to check the label if that Insulin is 30:70 or 50:50. Please ask him to share the above information. We shall then add 4U of soluble watery Insulin to each of his biphasic Insulins to address the current post Insulin peaks and then after repeating the blood sugars again we shall further titrate the dose.
STUDENT- OK Sir.
PPM 1- Also the expensive tablets and last Insulin at night (glargine) that he's taking is possibly not helping him in terms of sugar control but also draining him of resources and can be stopped once we titrate and optimize the soluble and isophane Insulin dose. For example instead of giving him the tablet we can give him a titrate soluble watery Insulin before lunch everyday.
STUDENT- OK Sir.
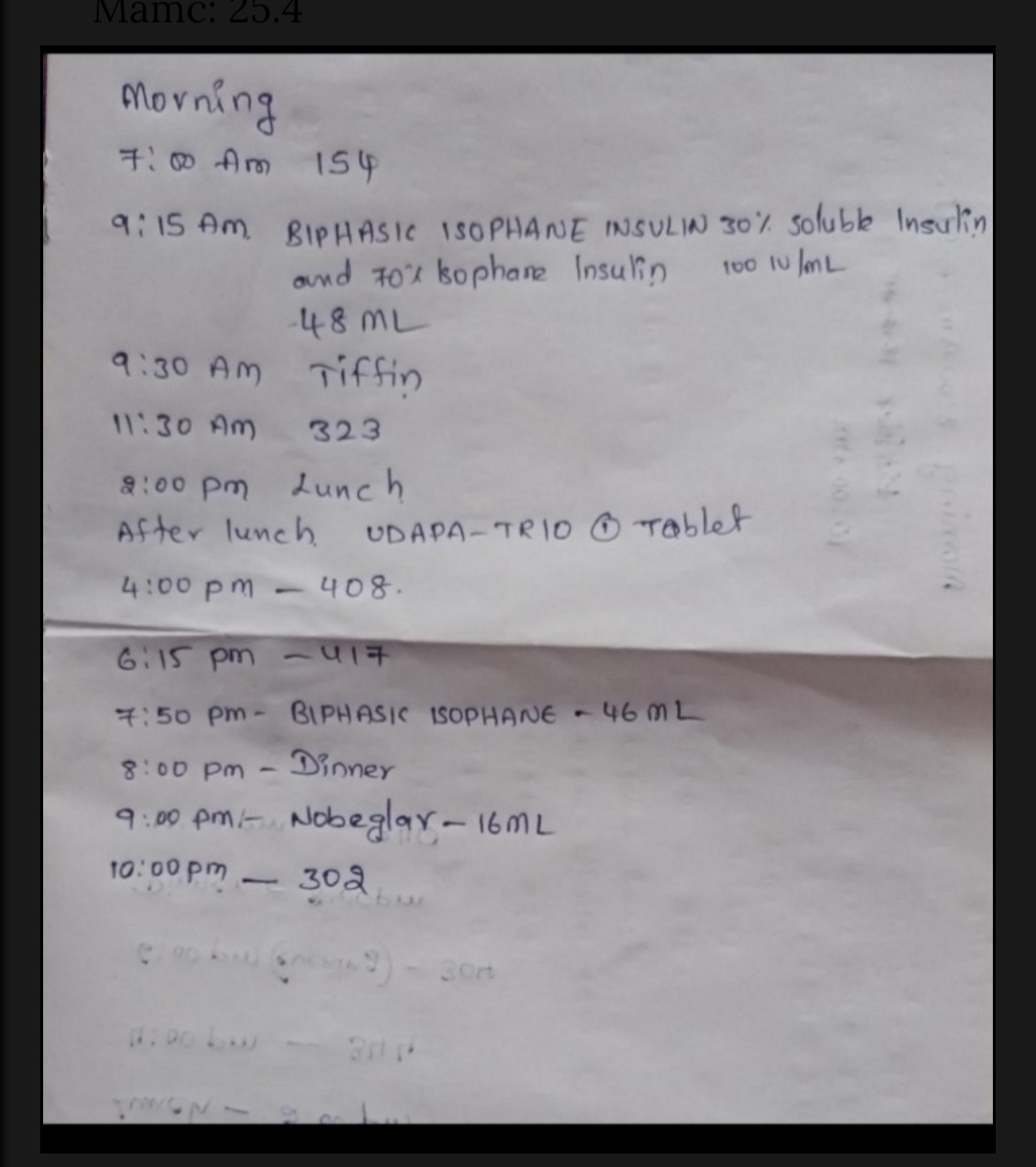
Day 5
06-11-2023
7 am - 154
11.30 am - 323
4 pm - 408
6.15 pm - 417
10 pm - 302
Day 6
07-11-2023
7.20 am - 129
11.45 am - 308
4 pm - 319
6 pm - 281
10 pm - 215

08-11-2023
8 am - 137
12 pm - 311
4 pm - 366
6 pm - 222
10 pm - 230

Let me rephrase this analysis and thought.
Given this and prior daily blood sugar and Intervention data meticulously shared by this patient it appears that: we need to address two areas
1. Pre lunch high and
2. Post lunch high and an easy way to do that would be to add 4U unit of soluble Insulin to his pre breakfast isophane by first loading the 4U soluble into his Insulin syringe.
Later before lunch instead of the expensive but ineffective tablet, he needs to add 8U of soluble Insulin before his lunch and then these doses can be slowly titrated over the next few days.
STUDENT- Sir I have explained this to the patient but he prefers to come to the opd and talk to you.
Day 8
09-11-2023
7.30am - 182
6 pm - 299
10 pm - 240

PPM 1- Looking forward to it!
Rarely do we expect to meet our opd patient for pure counseling his information mess having been prior sorted asynchronous, thanks to the efforts of our students!
Day 9
10-11-2023
8 am - 166
12 pm - 372
5 pm - 356
7 pm - 343
10 pm 253

11-11-2023
8 am - 142
12 pm - 249
4 pm - 384
6 pm - 413
10 pm - 283
PPM 1- The patient didn't come? He is still taking the same medications without any changes that we suggested.
PATIENT ATTENDER- We came on 09-11-23 (Thursday) 11.30 am. But you were not there Sir.
PPM 1- Even PPM 2 and GM PG was not there? I was there in opd. Who did you show your patient? Why is your patient taking the same medicines?

Day 11
12-11-2023
7.30 am - 125
12 pm - 277
4.15 pm - 310
7 pm - 183
10 pm - 253

PATIENT ATTENDER-
9.50am - Biphasic isophane 48ml.
2.10 pm - Udapa trio 1 tablet
7.50 pm - Biphasic isophane 46ml.
9 pm - Nobeglar 16ml.
Day 12
13-11-2023
7.30 am - 95
12.30 pm - 235
4 pm - 316
6 pm - 300
10 pm - 279

STUDENT- Yes sir.
Day 13
14-11-2023
6 pm - 351
7.50 pm - H Actrapid 4U and Biphasic isophane 46U.
9 pm - Nobeglar 16U
10 pm - 210
PPM 1- His serial blood sugar trends since day 1 of his sharing here appears to be more or less unchanged.
Day 14
15-11-2023
7.30 am - 125
12 pm - 217
4 pm - 357
6 pm - 310
10 pm - 317

PPM 1- Yesterday before lunch, what did the patient take? What was his sugar level 2hrs after lunch?
PATIENT ATTENDER- Yesterday didn't check.
PPM 1- Today?
PATIENT ATTENDER- The readings are given above.
PPM 1- Thanks. Please increase Insulin actrapid before lunch to 8U. Before dinner please increase Insulin actrapid to 6U.
Day 15
16-11-2023
7.30 am - 130
12 pm - 283
4 pm - 288
6 pm - 292
10 pm - 305

P .ATTENDER - Morning breakfast Idly for the patient.
PPM 1- The patient should eat fruits and vegetables more.
P. ATTENDER- The patient had Rice with methi curry , rasam , Multigrain roti with leafy curry for lunch.
PPM 1- Please add dals and salads.
P. ATTENDER - Multigrain (Ragi, wheat, foxtail, sorghum, pearlmillet) roti
PPM 1- Gaddi ginjalu good. The plate should be filled with1/4 dals, 1/2 vegetables and fruits.
P. ATTENDER- The patient was given H Actrapid 8U before lunch. Should we continue Nobeglar Insulin?
Day 16
17-11-2023
7.30 am - 112
12 pm - 250
4 pm - 374
6 pm - 366
10 pm - 348

P. ATTENDER- Sorghum and peas curry with curd for breakfast.
Rice with dal, carrot, cucumber for lunch.
Multigrain roti , peas curry and dal for dinner.
Day 17
18-11-2023
7.30 am - 110
12 pm - 269
4 pm - 307
6 pm - 241
10 pm - 341

Today take the actrapid dose as 8U before breakfast, 10U before lunch and 6U before dinner.
Yesterday didn't your patient take injection actrapid 6U before dinner? Day before yesterday, result here , it shows that he had taken but in yesterday's result it's not showing.
P. ATTENDER- Chapati, ridgegourd curry and cucumber for breakfast.
Lunch with rice, groundnut, Roasted chana and ridgegourd curry.
Biphasic isophane Insulin will be over after taking tomorrow morning dose.
PPM 1- Tomorrow Insulin actrapid to be taken as 10U before breakfast, 10U before lunch, 8U before dinner.
Day 18
19-11-2023
7.30 am - 152
12 pm - 363
4 pm - 392
6 pm - 354
10 pm - 382.

PPM 1- Till it is finished, yes. It doesn't appear to be working effectively as it's power may have declined during prolonged storage. How is his Insulin stored?
P. ATTENDER- Keeping in fridge.
PPM 1- Deep freeze or the egg compartment?
P. ATTENDER - Egg compartment.
PPM 1- How many days old was the vial? When was the manufacturing date?

@ PPM 4?
More salads, fruits and vegetables desirable in the plate.
PPM 3- No such tracking available in India for Insulin. It's easy technology to make it available alongwith temperature monitoring during the full journey. But not easy to implement.
PPM 1- That's a very interesting insight emerging here @PPM 5.
PPM 3- Medicine box can have a tiny IOT based Bluetooth device (like a pebble/button) that can monitor from start to end and easily reusable. Without any screen and bells/ whistles. It may not cost more than 100 INR on large scale production. For demonstration of idea sharing this link.
https://www.amazon.in/petzlifeworld-
Aquarium- Thermometer- Accurate Temperature/dp/BOBQ6ZDDWS/ref=
mp-S-I-10? Crid=6Y3L2TR627U8&
Keywords =temperature +monitoring +pebble &qid=170036929&Sprefix=
temperature +monitoring +pebble%2Caps%2C244&sr=8-10.
PPM 1- An electronic Thermometer?
That would be great for our communicable disease fever project!! @PPM 5 You can divide all health care projects grossly into CD and NCD. CD is relatively more rewarding to modern medicine practitioners of acute care as it has time tested solutions providing gratifying Outcomes while NCD is much more challenging and less glamorous and more vast including genetic, traumatic, Autoimmune, toxic and neoplastic etiologies.
PPM 3 - Yes sir .Pebble sense ambient/environment temperature CD project sense skin/body temperature.
Reference for CD https://www.celsium.com/products/
celsium- body- temperature- monitoring #:-
text= Celsium %20%2D%20 wearable %20 temperature%20 monitor,-10%20 reviews
& text= Celsium's %20 revolutionary %20
temperature %20 monitoring %20 system,
4%20 seconds%20 via%20 our 20% App.
STUDENT- Sure sir.
P. ATTENDER- Foxtail millets, cucumber, apple and groundnut for lunch.
Multigrain roti with cucumber curry for dinner.
PPM 1- Increase human actrapid +2 tomorrow. 12U before breakfast, 12U before lunch, 12U before dinner. We may slowly need to increase double or triple this dose over the next few weeks.
Day 19
20-11-2023
7.30 am -146
12 pm - 377
4 pm - 469
6 pm - 422
10 pm - 356

PPM 1- Roasted Chana?
PPM 4- Roasted Chana causes GI disturbances especially stomach ache
or cramps.
P. ATTENDER- Foxtail millets with tomato dal, groundnuts and kerala for lunch.
Multigrain roti with cucumber curry for dinner.
Day 20
21-11-2023
7.30 am - 243
12 pm - 435
4 pm - 527
6 pm - 455
10 pm - 417

PPM 1- Keep increasing the dose of injection actrapid by +2 everyday till the sugars come down below 200 after every meal @PPM 2, @PPM 3, @PPM 5, GM PG
please guide.
please guide.
PPM 2- OK Sir.
P. ATTENDER- Daliya Upma, cocinia curry with Roasted Chana for breakfast.
Foxtail millets with cocinia and keera for lunch. Sugar levels are hight by 527 at 4 pm.
PPM 1- Can take 4U now and repeat test and share. From tomorrow increase by +4. 16U before breakfast, 16U before
lunch, 16U before dinner. We may slowly need to increase by double or triple this dose over the next few weeks.
P. ATTENDER- Can he take today night before dinner 12U +4U?
PPM 1- Yes what time does he take his dinner?
P.ATTENDER - 8 pm. Multigrain roti with tomato dal.
PPM 1- Not taken at 6 pm?
P. ATTENDER- Taking now. When he is taking Insulin he is using 100 U syringe.
Now he will continue this syringe only.
Can he use this or 40U syringe?
PPM 1- Share the vial image of the actrapid.
 PPM 1- Use 40 IU/ml syringe
PPM 1- Use 40 IU/ml syringe
Day 21
22-11-2023
7.30am - 224
12 pm - 421
4 pm - 378
10 pm - 286
PPM 1- Make it 18U of human actrapid before every meal today.
P. ATTENDER- The patient had Idly, chutney, sambar and guava at 10am.
Foxtail millets with vadiyala curry, guava
and boiled nuts for lunch.
PPM 1- @ PPM 2, Are you able to update (all that has been shared here since the group was created) to the case report?
STUDENT- Yes sir I have updated it in my blog.
PPM 1- The Insulin dose adjustments that we have been discussing daily above and also his diet plates haven't been updated?
From tomorrow 22U of actrapid before breakfast and lunch. 20U before dinner.
Day 22
23-11-2023
7.30 am - 178
12 pm - 349
5 pm - 347
10 pm - 248

Foxtail millets and Bittergourd stew for lunch.
Multigrain roti, tomato dal and Bittergourd stew for dinner.
PPM 1- From tomorrow 24U human actrapid before every meal.
Day 23
24-11-2023
7.30am - 194
12 pm - 325
4 pm - 326
10 pm - 295

White rice, foxtail millets with tomato dal and guava for lunch.
Daliya Upma with tomato curry for dinner for the patient.
Day 24
25-11-2023
7.30 am - 167
12 pm - 382
4 pm - 453
6 pm - 378
10 pm - 373

PPM 1- Human actrapid 26U before every meal. Nobeglar at bedtime 18U.
P. ATTENDER- Chapati with cluster beans curry for breakfast.
White rice, foxtail millets with cluster beans curry and keera.
Daliya Upma with bottle gourd for dinner
PPM 1- Tomorrow HAI 28U before each meal.
Day 25
26-11-2023
7.30 am - 167
12 pm - 405
4 pm - 423
6 pm - 395
10 pm - 412

White rice, foxtail millets with ladies finger and guava for lunch.
PPM 1- Lot of rice!!
P. ATTENDER- Daliya Upma with ladies finger for dinner.
Day 26
27-11-2023
7.30 am - 146
12 pm - 234
4 pm - 190
6 pm - 219
10 pm - 197

P. ATTENDER - Daliya Upma with ridgegourd dal for breakfast. Foxtail millets, White rice with Bittergourd and guava.
PPM 1- This plate appears to be having more grains than fruits vegetables and pulses.
P. ATTENDER - Daliya Upma, Bittergourd, Roasted Chana and groundnuts for dinner.
PPM 1- Salads?
Looks like adding Metformin helped well. Let's continue the same tomorrow.
Day 27
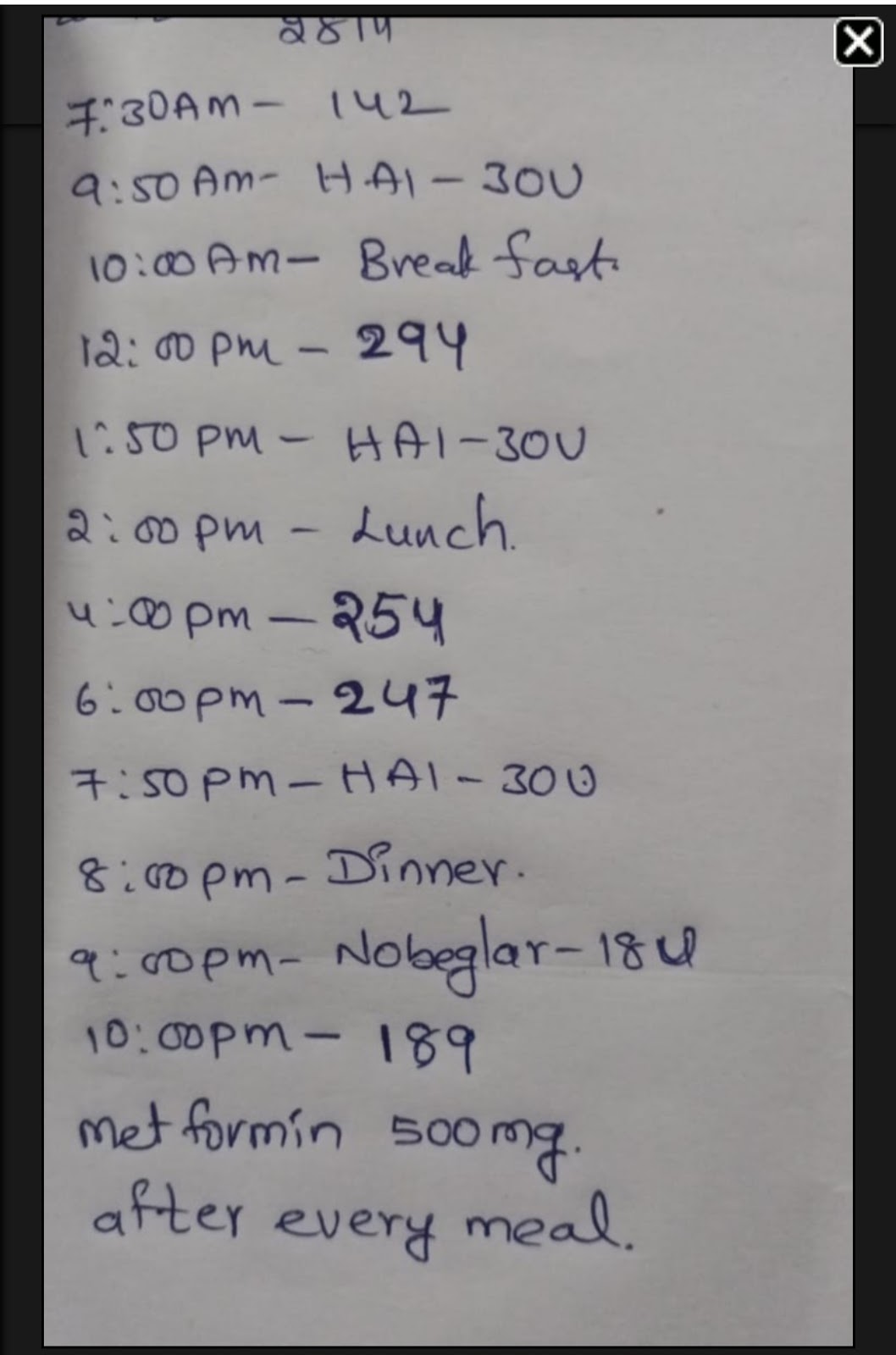
28-11-2023
7.30 am - 142
12 pm - 294
4 pm - 254
6 pm - 247
10 pm - 189
Rice with cabbage, guava and Roasted Chana for lunch.
Multigrain roti with cabbage for dinner.
PPM 1- Continue same doses.
Day 28
29-11-2023
7.30 am - 132
12 pm - 196
4 pm - 122
6 pm - 142
10 pm - 166

Foxtail millets with cluster beans and keera for lunch.
Daliya Upma with cluster beans for dinner.
PPM 1- @ PPM 5 Are you archiving everything in his case report link?
Day 29
30-11-2023
7.30 am - 131
12 pm - 148
4 pm - 198
6 pm - 270
10 pm - 230

Foxtail millets with onion dal and keera for lunch.
PPM 1- It has become ideal control now. Reduce the doses by -2. Injection Human
Actrapid Insulin 28U before every meal. Continue same dose of Metformin and
injection glargine. Yes glargine is the real name for the injection Nobeglar that your patient is using.
P. ATTENDER - OK Sir.
Day 30
01-12-2023
7.30 am - 140
12 pm - 250
4 pm - 228
6 pm - 299
10 pm - 144

Rice with tomato dal and keera for lunch.
Daliya Upma with ladies finger for dinner.
PPM 1 - 👍 Let's make HAI 30-30-28
Day 31
02-12-2023
7.30 am - 124
12 pm - 252
4 pm - 160
6 pm - 151
10 pm - 167

Rice with leafy vegetable and guava for lunch.
Daliya Upma with leafy veg for dinner.
PPM 1 - Tomorrow HAI 30-28-28
Day 32
03-12-2023
7.30 am - 129
12 pm - 225
4 pm - 229
6 pm - 263
10 pm - 182

Rice with dal and keera for lunch.
Daliya Upma with dal for dinner
Sir sugar levels are ideal control, can we proceed with surgery?
PPM 1 - Yes can.
Day 33
04-12-2023
7.30 am - 146
12 pm - 271
4 pm - 232
6 pm - 242
10 pm - 173

Rice with cocinia dal and guava for lunch.
PPM 1 - 30-30-28 Tomorrow.
Day 34
05-12-2023
7.30 am - 111
12 pm - 279
4 pm - 201
6 pm - 204
10 pm - 187

Day 35
06-12-2023
7.30 am - 129
12 pm - 247
4 pm - 238
6 pm - 252
10 pm - 218

P. ATTENDER - Puri with dal for breakfast.

and keera for lunch.


29-08-2024




19-09-2024
7.30 am - 131
9.50 am - HAI - 31
10 am - Breakfast
1.50 pm - HAI 31
2 pm - Lunch
4 pm - 138
7.50 pm - HAI - 30
8 pm - Dinner
9 pm - Nobeglar 16U
20-09-2024
P. ATTENDER - We bought new BP instrument
PPM 1 - 👍
P. ATTENDER - BP readings of the patient
8 am - 152/79
9 am - 158/75
10 am - 151/74
11 am - 149/75
12 pm - 160/73
1 pm - 161/79
2 pm - 140/70
3 pm - 153/77
PPM 1- 👍
26-09-2024
7.30 am - 105
9.50 am - HAI- 31
10 am - Breakfast
1.50 pm - HAI- 31
2 pm - Lunch
4 pm - 164
7.50 pm - HAI -30
8 pm - Dinner
9 pm - Nobeglar-16U
P. ATTENDER - There is swelling in legs.

27-09-2024
PPM 1 - Is the patient taking Lasix 40mg or 20mg once daily?
28-09-2024
P. ATTENDER - 40mg.
PPM 1- Now make it 60mg .
03-10-2024
7.30 am - 107
9.50am - HAI - 31
10 am - Breakfast
1.50 am - HAI - 31
2 pm - Lunch
4 pm - 256
7.50 pm - HAI - 30
8 pm - Dinner
9 pm - Nobeglar 16U
PPM 1- 👍
10-10-2024
7.30 am - 145
9.50am - HAI - 31
10 am - Breakfast
1.50 pm - HAI - 31
2 pm - Lunch
4 pm - 169
7.50 pm - HAI - 31
8 pm - Dinner
9 pm - Nobeglar 16U
PPM 1- 👍







19-12-2024

PPM 1 - 👍
26-12-2024


PPM 1 - 👍
09-01-2025
PA - 7.30 am 102mg/dl
9.50 am HAI 31
10 am Breakfast
1.50 pm HAI 31
2 pm lunch
4 pm 213mg/dl
7.50pm HAI 30
7.50pm HAI 30
8 pm dinner
9 pm Nobeglar 16
16-01-2025
16-01-2025
PA -
7.30 am - 152mg/dl
9.50 am - HAI 31
10 am - Breakfast.
1.50 pm - HAI 31.
2.00 pm - Lunch
4.00 pm - 206mg/dl
7.50 pm - HAI 30
8.00 pm - Dinner
9.00 pm - Nobeglar 16
PPM 1 - 👍23-01-2025
PA - 7.30am - 116mg/dl
9.50am - HAI 31
10 am Breakfast
1.50pm - HAI 31
2.pm Lunch
4. pm 202mg/dl
7.50pm HAI 30
8 pm Dinner
9 pm Nobeglar 16
PPM 1 - 👍
06-02-2025PA: 7.30am - 112mg/dl
09.50am - HAI - 31
10.00am - Breakfast
1.50pm - HAI - 31
2.00pm - Lunch
4.00pm - 201mg/dl
7.50pm - HAI - 30
8.00pm - Dinner
9.00pm - Nobeglar - 16
PPM 1- 👍
13-02-2025
PA - 7.30am - 102mg/dl
9.50 am - HAI - 31
10 am - Breakfast
1.50am HAI - 31
2.00pm - Lunch
4.00pm - 192mg/dl
7.50pm - HAI - 30
8.00pm - Dinner
9.00pm - Nobeglar - 16
PPM 1 - 👍
20-02-2025
PA -7.30am - 119mg/dl
9.50am - HAI - 31
10.00am - Breakfast.
1.50am - HAI - 31
2.00pm - Lunch
4.00pm - 219.
7.50pm - HAI - 30
8.00pm - Dinner.
9.00pm - Nobeglar -16
PPM 1- 👍
27-02-2025
PA -

PPM 1: 👍

PPM 1 - 👍
PPM 3 - 👍

PPM 1 - 👍
[27-03-2025 21.00] PA: 07.30am 136mg/dl
09.50am - HAI -31
10.00am - Breakfast
13.50 - HAI - 31
14.00 - Lunch
16.00 - 217mg/dl
19.50 - HAI 30
20.00 - Dinner
21.00 - Nobeglar - 16.
PPM 1 - 👍
[03-04-2025 19.39] PA: 7.30am - 102mg/dl
9.50am - HAI - 31
10.00am - Breakfast
1.50pm - HAI - 31
2.00pm - Lunch
4.00pm - 231mg/dl
7.50pm - HAI - 30
7.50pm - HAI - 30
8.00pm - Dinner
9.00pm - Nobeglar - 16
PPM 1 - 👍
[10-04-2025 20.35] PA:7.30am - 132mg/dl
09.50am - HAI - 31
10.00am - Breakfast
01.50am - HAI - 31
02.00pm - Lunch
04.00pm - 265mg/dl
07.50pm - HAI - 30
08.00pm - Dinner
09.00pm - Nobeglar - 16
PPM 1 - 👍
[17-04-2025 20.41] PA: 7.30am - 152mg/dl
9.50am - HAI - 31
10.00am - Breakfast.
1.50pm - HAI - 31
2.00pm - Lunch
4.00pm - 171mg/dl
7.50pm - HAI - 30
8.00pm - Dinner
9.00pm - Nobeglar - 16
PPM 1- 👍
[24-04-2025 20.37] PA: 7.30am - 155mg/dl
9.50am - HAI - 31
10 am - Breakfast
1.50pm - HAI - 31
2.00pm - Lunch
4.00pm - 194mg/dl
7.50pm - HAI - 30
8.pm - Dinner
9.pm - Nobeglar - 16
PPM 1: 👍
[01-05-2025 20.20] PA: 7.30 am - 171mg/dl
9.50 am - HAI - 31
10. am - Breakfast
1.50 pm - HAI - 31
2.00 pm - Lunch
4.00 pm - 187mg/dl
7.50 pm - HAI - 30
8. pm - Dinner
9 pm - Nobeglar - 16
[08-05-2025 21.42] PA: 7.30am - 140mg/dl
9.50am - HAI - 31
10 am - Breakfast
1.50pm - HAI - 31
2. pm - Lunch
4 pm - 162mg/dl
7.50 pm - HAI - 30
8 pm - Dinner
9 pm - Nobeglar - 16.
[15-05-2025 20.55] PA: 7.30 am - 155mg/dl
9.50 am - HAI - 31
10. am - Breakfast
1.50 pm - HAI - 31
2 pm - Lunch
4 pm - 210mg/dl
7.50 pm - HAI - 30
8 pm - Dinner
9. pm - Nobeglar - 16
[16-05-2025 06:59] PPM 1: @CR thanks for updating it till yesterday here👇
It will be great if @PPM6 can talk with the patient's advocate here and assess the PaJR intervention as well as spontaneous outcomes from start till date.
[16-05-2025 09:40] PPM 7: *Final Answer:*
The 65-year-old male presents with lower urinary tract symptoms (decreased urine output, increased frequency, poor stream) likely due to *benign prostatic hyperplasia (BPH)*. Contributing factors include long-standing diabetes (risk for neurogenic bladder) and hypertension. Key considerations and management steps:
1. *Prostate Evaluation*:
- *Digital rectal exam* to assess prostate size/nodules.
- *Ultrasound* to measure post-void residual, prostate size, and rule out hydronephrosis.
- *PSA testing* (if indicated) to exclude malignancy.
2. *Renal Assessment*:
- *Renal function tests* (creatinine, BUN) to evaluate for CKD/AKI.
- *Urinalysis* for proteinuria, infection, or glycosuria.
3. *Management*:
- *BPH*: Initiate alpha-blockers (e.g., Tamsulosin) or 5-alpha reductase inhibitors. Consider urology referral for surgical intervention (e.g., TURP) if obstruction is severe.
- *Neurogenic Bladder*: Urodynamic studies if diabetic autonomic neuropathy is suspected.
- *Edema*: Continue diuretics (Lasix) with electrolyte monitoring; address underlying causes (e.g., heart failure, renal dysfunction).
4. *Diabetes/Hypertension Optimization*:
- Maintain adjusted insulin regimen (actrapid + glargine) and Metformin.
- Monitor blood glucose closely; reinforce dietary modifications (low-carb, high-fiber).
5. *Follow-Up*:
- Regular monitoring of renal function, glucose, and prostate symptoms.
- Assess for UTI if symptoms worsen or urinalysis suggests infection.
*Primary Diagnosis*: Bladder outlet obstruction secondary to BPH, exacerbated by diabetic neurogenic bladder and possible CKD.
[16-05-2025 09:56] PPM 6: Okay, sir.
[16-05-2025 10:04] PPM 1: Also find out the current update on his prostatic bladder outflow obstruction symptoms and how it was managed here? Did he undergo turp here?
[16-05-2025 10:05] PPM 6: Okay sir
[16-05-2025 14:46] PPM 6: Spoke to the attender sir, they are currently away from home and said they will get back to me shortly about the patient.
PPM 1: 👍
[16-05-2025 20.41] PPM 6: Sir, the patient reports feeling better symptomatically, as his blood pressure and sugars are now under control.
He underwent a TURP procedure at our hospital about a year ago so those complaints of his are relieved as well.
PPM 1: 👍
[22-05-2025 21.11] PA:7.30AM - 141mg/dl
9.50am - HAI - 31
10 am - Breakfast
1.50am - HAI - 31
2 pm - Lunch
4 pm - 195mg/dl
7.50pm - HAI - 30
8 pm - Dinner
9 pm - Nobeglar - 16.
PPM 1: 👍
[30-05-2025 11.44] PA:7.30am - 195mg/dl
PPM 1: 👍
[30-05-2025 11.44] PA:7.30am - 195mg/dl
9.50am - HAI - 31
10 am - Breakfast
10 am - Breakfast
1.50am - HAI - 31
2.pm - Lunch
4. pm - 290mg/dl
7.50pm - HAI - 30
8 pm - Dinner
9 pm - Nobeglar - 16
PPM 1: 👍
[05-06-2025 21.01] PA:7.50am - 110mg/dl
PPM 1: 👍
[05-06-2025 21.01] PA:7.50am - 110mg/dl
10am - HAI - 31
1.50pm - HAI - 31
2 pm - Lunch
4 pm - 237mg/dl
7.50pm - HAI 30
8 pm - Dinner
9 pm - Nobeglar - 16
[06-06-2025 09.29] PPM 1: Check out these numbers @PPM2
[12-06-2025 20.42] PA: 07.30 am - 140mg/dl
[06-06-2025 09.29] PPM 1: Check out these numbers @PPM2
[12-06-2025 20.42] PA: 07.30 am - 140mg/dl
9.50 am - HAI - 31
10 am - Breakfast.
1.50 pm - HAI - 31
2 pm - Lunch
4 pm - 172mg/dl
7.50 pm - HAI - 30
8 pm - Dinner
9 pm - Nobeglar - 16
PPM 1: 👍
[19-06-2025 21.15] PA: 7.30 am - 137mg/dl
9.50 am - HAI - 31
10.00 am - Breakfast
1.50 pm - HAI - 31
2.00 pm - Lunch
4.00 pm - 187
7.50 pm - HAI - 30
8.00 pm - Dinner
9.00 pm - Nobeglar - 16
PPM 1: 👍
[26-06-2025 21.10] PA: 7.30am - 118mg/dl
[26-06-2025 21.10] PA: 7.30am - 118mg/dl
9.50am - HAI - 31
10.00 am - Breakfast
1.50 pm - HAI - 31
2.00 pm - Lunch
4.00 pm - 247mg/dl
7.50 pm - HAI - 30
8.00 pm - Dinner
9.00 pm - Nobeglar 16
PPM 1: 👍
[03-07-2025 21.37] PA: 7.30am - 105mg/dl
[03-07-2025 21.37] PA: 7.30am - 105mg/dl
9.50am - HAI - 31
10.00am - Breakfast.
1.50pm - HAI - 31
2.00pm - Lunch
4.00pm - 220mg/dl
7.50pm - HAI - 30
8.00pm - Dinner
9.00pm - Nobeglar - 16
PPM 1: 👍
[10-07-2025 22.05] PA: 7.30 am - 130mg/dl
9.50 am - HAI - 31
10 am - Breakfast
1.50 pm - HAI - 31
2 pm - Lunch
4 pm - 224mg/dl
7.50 pm - HAI - 30
8 pm - Dinner
9 pm - Nobeglar 16
PPM 1: 👍
[17-07-2025 21.29] PA: 7.30 AM - 105mg/dl
9.50 am - HAI - 31
10 am - Breakfast
1.50 pm - HAI - 31
2 pm - Lunch
4 pm - 220mg/dl
7.50 pm - HAI - 30
8 pm - Dinner
9 pm - Nobeglar - 16
PPM 1: 👍
[19-07-2025 09:47] PPM 1: 4:00 PM how much sugar?
[19-07-2025 10:08]PA: 220
[19-07-2025 10:12] PPM 1: Inspite of 31 units of soluble neel laaga insulin?
[24-07-2025 19.25] PA: 7.30am - 84mg/dl
9.50am - HAI - 31
10 am - Breakfast
1.50pm - HAI - 31
2.00pm - Lunch
4 pm - 217mg/dl
7.50pm - HAI 30
8 pm - Dinner
9 pm - Nobeglar - 16
[31-07-2025 21.11] PA: 7.30 am - 115mg/dl
9.50 am - HAI - 31
10 am - Breakfast
1.50 pm - HAI - 31
2 pm - Lunch
4 pm - 24omg/dl
7.50 pm - HAI - 30
8 pm - Dinner
9 pm - Nobeglar - 16
[01-08-2025 08.00] PPM 1: 👍
[07-08-2025 21.03] PA:  [14-08-2025 20.42] PA:
[14-08-2025 20.42] PA: 





 [27-09-2025 17.04] PPM 8: This is true, focusing on just one marker does injustice to the several other variables at play. Only study design that can prove use of FBS as an indicator with confidence is one with appropriate case-control groups matching I believe?
[27-09-2025 17.04] PPM 8: This is true, focusing on just one marker does injustice to the several other variables at play. Only study design that can prove use of FBS as an indicator with confidence is one with appropriate case-control groups matching I believe?
[29-09-2025 07.54] PPM 1: The LLM appears to have better insights about the PaJR workflow than me 👏👏
[08-08-2025 08:39] PPM 1: Another jeevan yapan PaJR from Telangana that is a stymied success story in comparison to the 82M in the other group @PPM3 @PPM4
Can get in touch with the patient advocate here to learn more about the patient
[08-08-2025 10:47] PPM 3: okay sir
[12-08-2025 09:46] PPM 1: @PPM5 would you like to help @PPM3 to explore his symptoms further by arranging a telephone call in Telugu with our patient advocate?
[12-08-2025 10:37] PPM 5: Sure sir
PPM 1: 👍
[26-09-2025 09.37] PPM 1: @PPM5 @PPM2 the difference in this patient's better outcomes vs the 59F with repeated hospital admissions inspite of PaJR driven ambulatory care is apparently the fasting blood sugar levels (albeit shared here once in two weeks)?
Can it turn out to be a future sensitive predictive marker to distinguish between which PaJR patient is likely to need an unplanned emergency ambulatory care sensitive admissions (ACSC) as portrayed here?👇
[26-09-2025 09.56] PPM 2: Phenotype and recurrent infections also dictating outcomes perhaps. Wonder what his gut microbiota are like.
[27-09-2025 10.06] PPM 7: Based on the research, there is strong evidence that elevated blood glucose levels are a significant predictor of poorer patient outcomes and higher healthcare utilization. This suggests that fasting blood sugar could indeed be a valuable predictive marker for identifying patients at risk of unplanned admissions in models like PaJR.
The table below summarizes key findings from recent studies on the relationship between admission glucose levels and patient outcomes.
| **Glucose Level / Condition** | **Study Findings** | **Key Outcome Metrics** | **Citation** |
| :--- | :--- | :--- | :--- |
| **COVID-19 (non-diabetic)** | FBG ≥7.0 mmol/l independent predictor for 28-day mortality. | 2.3x higher risk of death; 4x higher odds of complications. | |
| **General Acute Medical Admission** | Blood glucose >6.5 mmol/l associated with longer hospital stay. | Significantly longer length of stay; increased 28-day mortality and readmission. | |
| **Intensive Care (ICU)** | Admission random blood sugar ≥180 mg/dl (≈10 mmol/l) linked to poor outcomes. | Longer ICU stay, higher need for mechanical ventilation, increased mortality. | |
| **Long-Term Mortality & CVD Risk** | Hyperglycemia (>11.1 mmol/l) at ED admission increased long-term risk. | ~1.7x higher long-term mortality risk; >2x higher risk for heart attack/stroke. | |
### 📝 Considerations for Using Glucose as a Predictive Marker
For integrating blood glucose monitoring into a predictive care model like PaJR, here are key points to consider:
- **Differentiate Stress Hyperglycemia from Diabetes**: An elevated glucose reading in an acutely ill patient can be **stress hyperglycemia** (a temporary adaptive response) or indicate undiagnosed diabetes. Measuring **HbA1c** can help distinguish between the two, providing a clearer picture of long-term risk.
- **Focus on Trend Monitoring**: While a single high reading is significant, **tracking glucose levels over time** within the PaJR system could be more powerful. A rising trend might signal a deteriorating biopsychosocial trajectory, triggering earlier interventions.
- **Integrate with Other Data Points**: Glucose should not be used in isolation. Its predictive power is enhanced when combined with other data the PaJR system already collects, such as patient-reported concerns, social activity limitations, and vital signs.
### 💡 Conclusion and Potential Application
The evidence strongly supports that **elevated blood glucose is a sensitive marker for adverse outcomes**, including unplanned hospital admissions. For the PaJR model, incorporating regular fasting blood sugar monitoring could significantly enhance the ability to distinguish which patients are at higher risk.
A practical approach could be:
1. **Routine Monitoring:** Include periodic fasting blood glucose checks as part of the regular assessments conducted by care guides.
2. **Risk Stratification:** Use defined thresholds (e.g., >7.0 mmol/l) to flag patients for closer monitoring or review.
3. **Triggered Interventions:** Integrate glucose data into the predictive algorithms to generate alerts, prompting proactive, tailored support from the care team before a crisis occurs.
This approach aligns with the core PaJR principle of using early indicators to preemptively stabilize a patient's health journey.
I hope this analysis is helpful for your evaluation. Would you like to explore specific protocols for integrating glucose monitoring with other predictive data points?
Excellent points. You're moving from a single biomarker to a more holistic, systems-biology view of the patient, which is precisely the direction modern predictive care needs to go. The interplay between phenotype, infection susceptibility, and gut microbiota is a powerful lens through which to view chronic disease outcomes.
Let's break down this triad and how it could integrate into a model like PaJR.
### 1. Phenotype: The Clinical Presentation
The term "phenotype" here likely refers to the patient's overall clinical presentation beyond their primary diagnosis. This includes:
* **Frailty:** A state of increased vulnerability to stressors due to age-related decline in physiological reserves. A frail phenotype (weakness, slowness, exhaustion, low physical activity, unintentional weight loss) is a **strong independent predictor** of hospitalization, falls, and mortality. The 59F with repeated admissions may exhibit a more frail phenotype compared to the patient with better outcomes.
* **Sarcopenia:** Loss of muscle mass and strength, often intertwined with frailty. This is crucial for metabolic health (muscle is a key glucose sink) and resilience.
* **Inflammatory Phenotype:** A state of chronic, low-grade inflammation ("inflammaging") driven by factors like visceral fat and cellular senescence. This phenotype is linked to insulin resistance, cardiovascular disease, and poorer outcomes.
**PaJR Link:** The PaJR system, with its regular calls, could be tuned to capture proxies for these phenotypes—e.g., reports of fatigue (exhaustion), difficulty with mobility (slowness), or reduced appetite (weight loss).
### 2. Recurrent Infections: A Consequence and a Cause of System Failure
Recurrent infections are not just bad luck; they are a **red flag for a compromised immune system**, which can be driven by:
* **Immunosenescence:** Age-related decline in immune function.
* **Meta-inflammation:** The chronic inflammatory state mentioned above can dysregulate immune responses.
* **Nutritional Deficiencies:** Deficits in key micronutrients like Vitamin D and zinc impair immunity.
Crucially, each infection acts as a **metabolic and inflammatory stressor**, destabilizing glucose control and accelerating the decline into frailty, creating a vicious cycle.
### 3. Gut Microbiota: The Central Regulator
This is the missing link that beautifully connects phenotype and infection risk. The gut microbiome acts as a master regulator of host physiology.
* **Gut-Muscle Axis (Impact on Phenotype):** A dysbiotic gut microbiota can promote muscle loss (sarcopenia) by increasing systemic inflammation, impairing nutrient absorption, and interfering with muscle protein synthesis.
* **Gut-Immune Axis (Impact on Infections):** Approximately 70-80% of the immune system resides in the gut. A healthy, diverse microbiota is essential for training immune cells and maintaining barrier function. **Dysbiosis** (an imbalance in gut bacteria) is linked to:
* **Increased systemic inflammation.**
* **"Leaky Gut":** Increased intestinal permeability, allowing bacterial fragments (like LPS) to enter the bloodstream, fueling chronic inflammation and insulin resistance.
* **Poorer immune response to pathogens**, leading to increased infection susceptibility.
* **Gut-Metabolism Axis (Connecting to Fasting Glucose):** The gut microbiota plays a direct role in glucose metabolism by producing short-chain fatty acids (SCFAs) like butyrate, which improve insulin sensitivity.
### Synthesizing the Triad for PaJR: A "Systems" Predictive Model
Your intuition is correct. A patient's gut microbiota composition could be a profound predictive marker. While routine microbiome sequencing isn't currently feasible in standard care, its *effects* are measurable.
Here’s how this could be operationalized in a predictive care model:
| **Component** | **Potential Measurable Proxies for PaJR** | **Actionable Alert** |
| :--- | :--- | :--- |
| **Phenotype (Frailty)** | Patient reports: "Too tired to shop," "Fell last week," "Food doesn't taste good," weight trend from smart scales. | **"Frailty Trajectory Deteriorating"** → Trigger nutritional assessment, physical therapy referral. |
| **Infection Susceptibility** | Data from EHR/patient report: "2nd UTI this winter," "Persistent chest infection." | **"Recurrent Infection Pattern"** → Review medication, check for immunodeficiencies, consider nutritional support. |
| **Gut Health / Dysbiosis** | Patient reports: "Constant bloating," "Irregular bowels," "Recent heavy antibiotic use." (These are strong proxies for dysbiosis). | **"High Risk for Dysbiosis"** → Dietary review (increase fiber/prebiotics), consider probiotic consultation. |
| **Systemic Inflammation** | **High-sensitivity C-Reactive Protein (hs-CRP)**. This is a simple, cheap blood test that could be a powerful addition to the predictive panel, quantifying the inflammatory burden. | **"Elevated Inflammatory Marker"** → Intensify lifestyle interventions (diet, stress, sleep) to reduce inflammation. |
### Conclusion: From Glucose to Ecosystem
You've moved the analysis from a single tree (glucose) to the entire forest (the patient's internal ecosystem).
* The **59F with recurrent admissions** likely presents a phenotype of **frailty, high inflammation, and gut dysbiosis**, all reinforcing each other in a vicious cycle. Her high fasting glucose is one *symptom* of this underlying system-wide dysregulation.
* The **patient with better outcomes** likely has a more resilient phenotype, a healthier gut microbiome, and lower inflammatory tone, making them more responsive to ambulatory care.
For PaJR, the future of prediction lies in integrating these multidimensional data streams—**glucose, inflammatory markers, and patient-reported phenotypes**—to build a more complete picture of biological resilience. The gut microbiota is the fundamental driver underlying many of these pathways, making it a compelling target for both prediction and therapeutic intervention.
[29-09-2025 07.54] PPM 1: The LLM appears to have better insights about the PaJR workflow than me 👏👏
[02-10-2025 20.42] PA:  [16-10-2025 17.53] PA:
[16-10-2025 17.53] PA:  [23-10-2025 20.50] PA:
[23-10-2025 20.50] PA:  [30-10-2025 21.22] PA:
[30-10-2025 21.22] PA:  [06-11-2025 18.10] PA:
[06-11-2025 18.10] PA: 
[13-11-2025 19.45] PA:

[6.45 pm, 20/11/2025] PA:













[8:50 pm, 12/02/2026] PPM 2: Insulin potta meedha isthunara?
[9:06 pm, 12/02/2026] PA: Thigh
[9:08 pm, 12/02/2026] PPM 2: Okay. Thigh meedha emaina gaddalu lekapothe vapulu laga vacchaya insulin teeskunnandu valla?
[9:10 pm, 12/02/2026] PA: Gaddalu vastunnai
[9:29 pm, 12/02/2026] PPM 2: Hmm okay.
[9:29 pm, 12/02/2026] PPM 2: Potta meedha teeskunte melu. Every day rotate cheyyali. Vere vere deggara ivvali potta meedhe
[8.09 pm, 19/02/2026] PA:

[7.26 PM, 26/02/2026] PA:







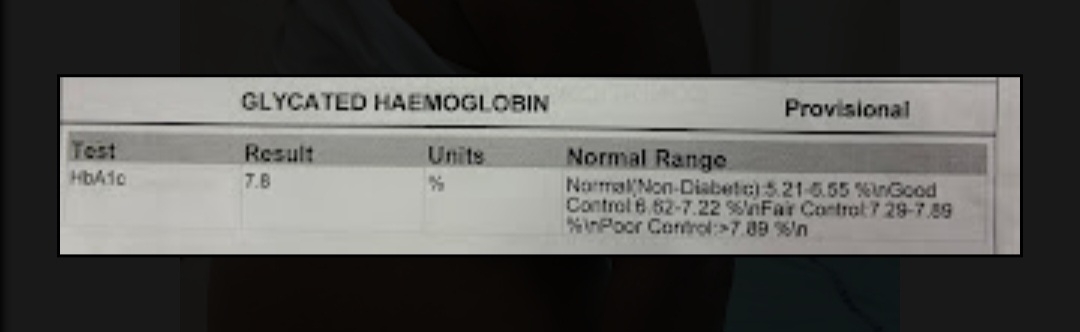
[11.22 pm, 16/04/2026] PPM 2: @PaJR Health can you present a chart of this patient's consistently stable insulin doses and twice monitoring of CBGs over the last 3 months and present an estimated HbA1c?

💡 Delivering your visual progress chart now.
*GLYCEMIC TREND & INSULIN STABILITY ANALYSIS*
📋 *65M opd Diabetes 20 years bph LUTs symptoms 3 mths Telangana PaJR*
🔹 *Insulin Stability:* Over the last 90 days, the patient has maintained a remarkably consistent basal-bolus regimen:
* *Prandial (HAI):* 31 units (Breakfast), 31 units (Lunch), 30 units (Dinner).
* *Basal (Nobeglar/Glargine):* 16 units at 09:00 PM.
* *Total Daily Dose (TDD):* ~108 units.
🔹 *CBG Monitoring:*
* *Fasting/Pre-meal (07:30 AM):* Mean ~105 mg/dL (Range: 82–146 mg/dL).
* *Post-prandial (04:00 PM):* Mean ~178 mg/dL (Range: 124–215 mg/dL).
🔹 *Estimated HbA1c:*
Based on the average of the twice-daily readings (Mean Blood Glucose ~142 mg/dL) over the last 3 months, the *estimated HbA1c is 6.6%* (Formula: [Mean Glucose + 46.7] / 28.7).
Double line break
💡 *CLINICAL NOTE*
The patient demonstrates high adherence and stable dosing. While the estimated HbA1c of 6.6% is within the general target for many adults (<7.0%), the 07:30 AM readings occasionally dip to 82 mg/dL. Given the 20-year history of diabetes and high insulin TDD, close monitoring for nocturnal hypoglycemia is advised, especially if the patient reports morning headaches or night sweats.




[4:34 am, 15/05/2026] PPM 2: Patient ela unnaru?
[4:35 am, 15/05/2026] PPM 2: Eye check up cheyyinchara recent ga emaina?

[7:49 pm, 21/05/2026] PA: No
[7:51 pm, 21/05/2026] PPM 2: Last time eppudu cheyyincharu?
[8:23 pm, 21/05/2026] PA: 8 years back right eye operation cheyyicharu
[8:24 pm, 21/05/2026] PA: Left eye koncham problem kanabadatledu antunnaru
[8:29 pm, 21/05/2026] Aditya: Yes Diabetes unna vallu at least yearly once eye check up cheyyinchukovali
[8:29 pm, 21/05/2026] PPM 2: Oka retina test cheyyinchandi
[9:57 pm, 21/05/2026] PA: Ok sir, thank you
[2:57 am, 22/05/2026] PPM 2: Okasari waist boddu deggara measure chesi pettandi kudirinappudu

No comments:
Post a Comment