
08-02-2025
This is an Online ELog Book to discuss our patient's de-identified health data shared after taking his signed informed consent. Here we discuss our patient's problems through series of inputs from available global online community experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
PPM 1 -
Afternoon session:
37M with sudden vomiting and giddiness since yesterday
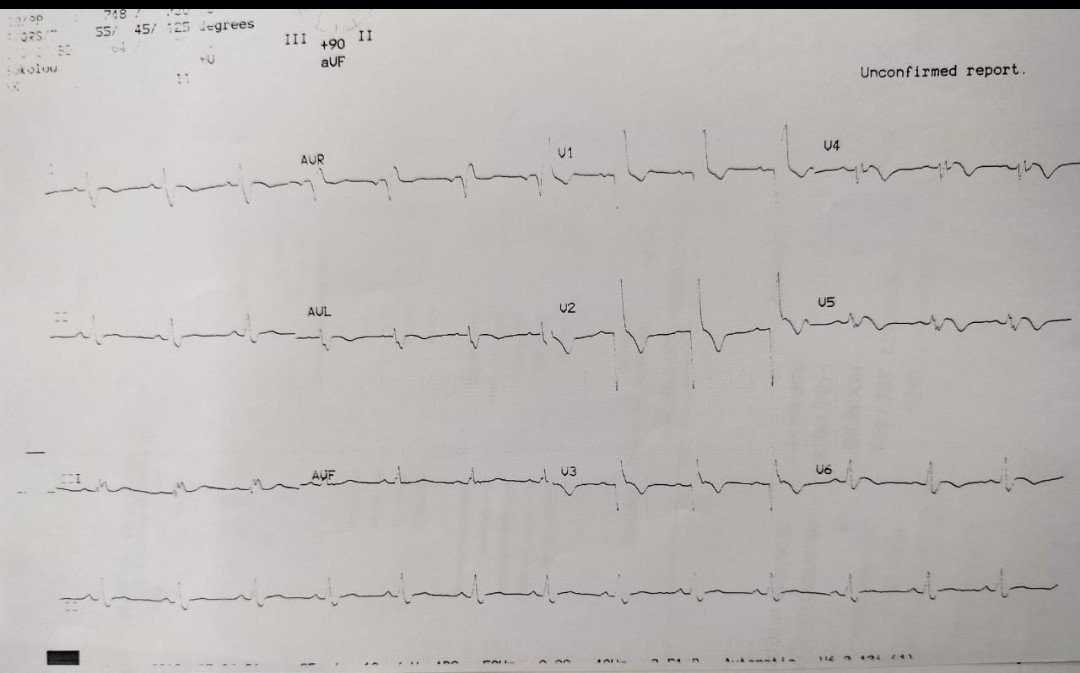
On 10th May, 2018 he developed chest pain radiating to throat and was brought here when the ECG showed...




This was his Echo at that time showing LAD akinesia and that appears to be persistent.


10-02-2025
PPM 1 - @PPM3 please share the update of this patient. I was busy in the ward with the other patients today but i was told that he was being seen by you and started on iv prophylactic valproate for raised ICT other than iv mannitol etc.
Just let me know what has been the changes in his CNS examination findings from friday till today @PPM3
PPM 3 - Sir after admission we have done an MRI in suspicion of PCA stroke and it turned out to be AIS large infarct involving b/l cerebellar hemispheres & vermis
Managed his AIS + CAD combinedly.
PPM 1 - AIS?
PPM 3 - Even though his vomiting subsided he stated complaining of severe headache since today morning and is a bit drowsy
O/E:
PR was fluctuating b/w 45 - 55 BPM
Apnea episodes were there in between with fall in SpO2 to 80 - 85%
PPM 1 - Can you share the MRI image showing that?
PPM 3 - So in suspicion of raised ICT (Reactive vasogenic edema) we gave him mannitol IV stat & started on 3% NACL infusion sir
Dexa & lasix were also given sir as a Rx for reactive vasogenic edema sir.
Yes sir
@PPM4 @PPM5 Plz share the MRI images.
PPM 1 - Good
What about prophylactic iv valproate? Is there any literature to suggest that it reduces incidence of Seizures in stroke with raised ICT patients?
PPM 3 - Reactive vasogenic cerebral edema typically intensifies over 3 to 4 days after the initial infarct.
Cerebellar strokes, especially after the first day, tend to develop progressive edema and potential subsequent herniation. Early symptoms often include severe headache, altered mental status, vomiting, and drowsiness. The important neurological signs for these patients are impaired level of consciousness, new or worsened cranial nerve deficits, gaze paresis, and downward gaze conjugation.
In the acute setting, temporary reduction of intracranial pressure can be achieved using agents like mannitol, hypertonic saline, or hyperventilation.
In cases of large strokes with significant cerebral edema, especially if the intracranial pressure is elevated, neurosurgical interventions such as extra ventricular drains, ventriculostomy, or decompressive suboccipital craniotomy may be necessary.
Neurosurgical procedures like removal of infarcted tissue or hematoma are occasionally required.
PPM 4 - 

Sir usually it's not indicated/recommended as a prophylaxis in case of ischemic strokes (although used in some neuro centres)
But there is some evidence of prophylactic antiepileptics in patients with traumatic brain injury sir.
Coming to this patient sir I have observed some jerky movements in left upper limb during my morning rounds which could be a focal seizure in the context of his neurological injury
So I started him on antiepileptic also sir
PPM 1 - 👍
Thanks. Good. Was the jerky movements documented in the file?
PPM 3 - 

No comments:
Post a Comment