
This is online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs .This e-log book also reflects my patient centered online learning portfolio and your valuable comments on comment box is welcome.
roll no: 55
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with a diagnosis and treatment plan.
Following is the view of my case:
40yr female came with chief complaints of
Weakness of both upper and lower limbs since 4 hours
History of present illness:
Patient was apparently asymptomatic hours ago then she is unable to get up from bed and walk properly. She has h/o 2 episodes of vomiting which are non bilious, non projectile, filled with food particles.
H/o similar complaints in the past
1st episode -3to 4 yrs back bad left lower limb weakness and was diagnosed to have hypokalemia for which potassium correction was done
2nd episode: in Nov 2021 had h/o both upper and lower limbs weakness , Loss of consciousness for 2 days , loss of speech (for 4 days) , 1 unit PRBC was transfused and was diagnosed as hypokalemia.
3rd episode : in may 2022 she had same complaints and was admitted for 3 days.
Not a k/c/o HTN, DM,CVA, CAD, EPILEPSY ,TB,ASTHMA.
Personal history:
Diet: mixed
Appetite:normal
Sleep: adequate
Bowel and bladder movements: regular
Addictions:none
Sequence of events:
She got married in 1999 and had her first child in 2002. H/O abortion in 2001.
Due to some issues she worked as a nurse at local hospital for 6 months.
Later her husband passed away in 2009 and in 2010 she got married again. Since then until 2019 she was alright with out any health problems.
1st episode in 2019
2nd episode in 2021
3rd episode in 2022
General examination:
Pt is conscious, coherent and cooperative
No pallor, icterus, cyanosis, clubbing, lymphadenopathy, pedal edema



Bp:100/60mmhg
Pr:90bpm
Rr:16cpm
Cvs:s1, s2 present
RS: BAE + , clear
CNS: HMF +
P/A : soft , non tender
Bowel sounds:sluggish
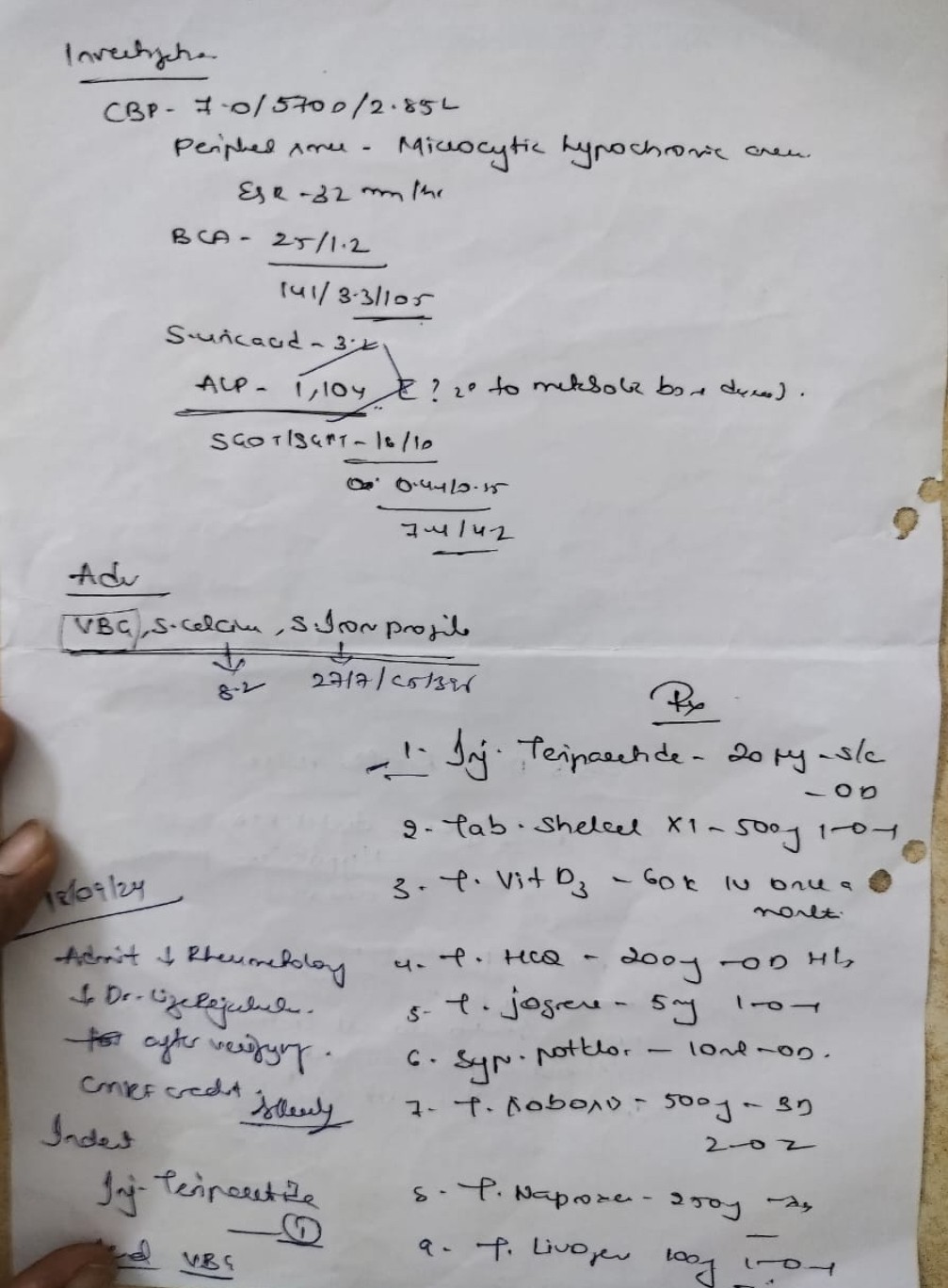
Investigations
Chest x ray

X ray B/L wrist


Serum electrolytes
Sodium:142
Potassium: 1.8
Chloride:108
Calcium ionized:1.35
Serum calcium:9.8
Serum creatinine:1.3
Blood urea:29
RBS:101
LFT:
Total bilirubin:0.60
Direct bilirubin:0.19
SGOT:11
SGPT:23
ALP:579
Total proteins: 4.8
Albumin: 2.95
A/G:1.59
Diagnosis:
Recurrent hypokalemic paralysis secondary to distal RTA and probable sjogrens
Treatment
IV fluids 1 NS and 1 RL @ 75ml/hr
Inj KCL 3 ampules (60mEq) in 500ml NS over 3 hours
Syrup potklor 15ml po/TID
Inj zofer 4mg IV/SOS
TAB PREGABA M 75mg po/hs
ECG 12th hourly
Investigations on 1/2/23
Urinary calcium:3.0
Spot urine sodium:60
Spot urinary potassium:12.0
Usg on 1/2/23
TIRADS 3 lesion in left lobe
TIRADS 4 and 1 lesion in right lobe
Parotitis of left side
Serum electrolytes on 2/2/23
Sodium:140
Potassium:3.8
Chloride:101
Calcium ionized:1.07
Thyroid profile on 1/2/23
T3:0.78
T4: 9.64
TSH:1.52
24 hr urinary electrolytes :
24 hr urinary potassium:55.6 (normal range:25-125)
24hr urinary sodium:552 (normal range:40-220)
24hr urine volume:4,600ml
X ray pelvis








👆 there's a urinary calcium mentioned here altogether not sure how useful that is




No comments:
Post a Comment