
18-11-2024
THIS IS AN ONLINE E LOG BOOK TO DISCUSS OUR PATIENT'S DE-IDENTIFIED HEALTH DATA SHARED AFTER TAKING HIS SIGNED INFORMED CONSENT. HERE WE DISCUSS OUR PATIENT'S PROBLEMS THROUGH SERIES OF INPUTS FROM AVAILABLE GLOBAL ONLINE COMMUNITY EXPERTS WITH AN AIM TO SOLVE THOSE PATIENTS CLINICAL PROBLEMS WITH COLLECTIVE CURRENT BEST EVIDENCE BASED INPUTS.


Our patient has come from 2000 km far and shared his problem that he Has:
1. Ulcer in the stomach detected by the local doctors
2. His brother went to Hyderabad last month
3. He is in serious condition
4. He is facing now blood- vomiting, stomach pain,
5. He is willing to go to Hyderabad very soon
The PHR, patient journey record PaJR transcripts below reflect the therapeutic uncertainties around the patient and their resolution through team based learning:
Here's the rest of the discussions not yet updated in the case report 👇
[11/19, 4:40 PM] PaJR PHR Moderator: 👆Baki ekhane chawa tottho guno o share korun
[11/19, 4:56 PM] 39 M Wb: Pet fule gechilo pa fule gechilo.khete parchilo na pore osudh khabar por fola kome geche kintu Navi ta fola ache onek ta.halka betha kore Navi ta












[11/19, 7:54 PM] PaJR PHR Moderator: Patient alcohol last kabe kheyechilen?
[11/19, 9:50 PM] 39 M Wb: 1 bochor age
[11/19, 10:06 PM] PaJR PHR Moderator: Aekhon peter fola aage theke komeche?
[11/19, 10:35 PM] 39 M Wb: Haa
[11/19, 10:40 PM] 39 M Wb s: Kintu Navi fola komea nai
[11/20, 8:08 AM] PaJR PHR Moderator: Last ultrasound kabe hoyechilo?
[11/20, 5:33 PM] 39 M Wb : 07/05/2023
[11/20, 6:28 PM] PaJR PHR Moderator: Tahole aekhon ekta ultrasound korle bojha jabe fola ta kono boro somosyar karone kina
[11/20, 6:55 PM] 39 M Wb : Ultrasound Amader Khane korte hobe
na ki Hyderabad
Jete hobe sir
[11/20, 8:50 PM] PaJR PHR Moderator: Okhane korleo habe
[11/20, 9:41 PM] 39 M Wb: Theek acche
[25-03-2025 22:33] PA: Sir nomoskar





















 [23-04-2025 15.47] PA: Sir apni jeta 15 din er jonno medicine diye chilen to ota sesh hoye gheche. Ekhon ki agher medicine ta change korbo naki otai continue calabo sir.
[23-04-2025 15.47] PA: Sir apni jeta 15 din er jonno medicine diye chilen to ota sesh hoye gheche. Ekhon ki agher medicine ta change korbo naki otai continue calabo sir.
[23-04-2025 19:37] PPM 1: Aeguno continue kore jaan Paa fola ta kemon chobi pathan

[23-04-2025 19.46] PA: Sir pha fula ta komche

[10-05-2025 21.01] PPM 1: Oshudh ki maajhe bondho chilo? Bortoman oshudh gunor chobi share korun






 [20-05-2025 18.23] PA: Ar Wait 57kg
[20-05-2025 18.23] PA: Ar Wait 57kg

[25-03-2025 22:34] PA: Sir patient ra aj train a uthe geche
[25-03-2025 22:53] S: Where is patient, is patient going tomorrow to our hospital?
[25-03-2025 22:56] PA: Patient porsu din jabe hospital
[26-03-2025 00:07] S: Please ask patient to call me if he needs any support 🙏
[28-03-2025 07:09] PA: Sir nomoskar
[28-03-2025 07:10] PA: Patient ra neme geche .
[28-03-2025 08:48] PPM 1: Thik achhe. Ami OPD te pahuchobo totokkhon OPD ticket ebong bhortir
kagoj ta baniye rakhben
[28-03-2025 08:52] S: Please ask patient to call me for any help needed to navigate in the hospital
[28-03-2025 08:52] S: হাসপাতালে যাতায়াতের জন্য যেকোনো সাহায্যের জন্য রোগীকে আমাকে ফোন করতে বলুন।
[28-03-2025 08:52] PPM 1: @CR this long distance patient is reaching our OPD today.
No case report link in the description box here yet I guess although the group was created by
@~PA @LB on November 2024. Will share his signed informed consent today.
along with the 18F for their case reports to be made.
[28-03-2025 08:54] PA: Sir onara kagoj banache.
[28-03-2025 09:42] PA: Sir patient der kagoj hoye geche .patient khub asustho.
[28-03-2025 09:43] PPM 1: Ami OPD r dike aegucchi
[28-03-2025 09:47] PPM 5: Needs a liver transplant.
[28-03-2025 10:10] PA: Ok sir
[28-03-2025 10:34] PPM 1: @~PPM6 @~PPM7 please add @PPM8 to the
group as she's the unit incharge right now evaluating this patient with us in the OPD


[28-03-2025 14:20] PA: Ok sir
[28-03-2025 16:30] PPM 1: Please crop out the identifiers and then share. Deleting it till then
[28-03-2025 16:30] PPM 9: Ok sir



[28-03-2025 20.06] PPM 9: ASCITIC TAP DONE 28/03/25
Abdominal girth
Before tap 104cm
After tap 101 cm
Body Weight
Before tap 70kgs
After tap 67 kgs
PPM 1: 👍


[29-03-2025 16:22] PPM 1: Afternoon session:
[29-03-2025 16:23] PPM 1: @~PPM3 @~PPM4 see if you can share the detailed history of this patient
also here
[29-03-2025 16:38] PPM 3: yes okay sir
[29-03-2025 16:48] PPM 4: Okay sir
[29-03-2025 18.44] PPM 9: 2nd day ascitic tap of 2litres

PPM 1 - 👍

PPM 1 - 👍

[01-04-2025 11.26] PPM 1: Investigations




[01-04-2025 15.51] PPM 1: 👍

[02-04-2025 15.51] PPM 1: Yesterday's TLC jumped from 3000 to 9000!

[02-04-2025 15.57] PPM 1: First fever spike yesterday following yesterday's ascitic tap!

[03-04-2025 08.58] PPM 9:


[03-04-2025 09:04] PPM 9: No fever spikes
[03-04-2025 10:38] PPM 1: Please share the updated fever chart and his ascitic fluid cell type and cell counts sent yesterday @~PPM10 @~PPM9
[03-04-2025 10:39] PPM 1: Let's not measure abdominal girth as it may not help anywhere close to daily weight record
[03-04-2025 10:41] PPM 1: @~PPM10 if the ascitic fluid counts come normal since day before yesterday when he developed the fever spike then the spike would be more likely to be due to his thrombophlebitis and the fever in thrombophlebitis comes down once the iv is removed. In that case our ceftriaxone too would be an overkill
[03-04-2025 13:32] PPM 10: I will update in 5 min sir
[03-04-2025 13:33] PPM 10: Yesterday they told that hod sir will see it and give report today
[03-04-2025 14:10] PPM 9: Ok sir
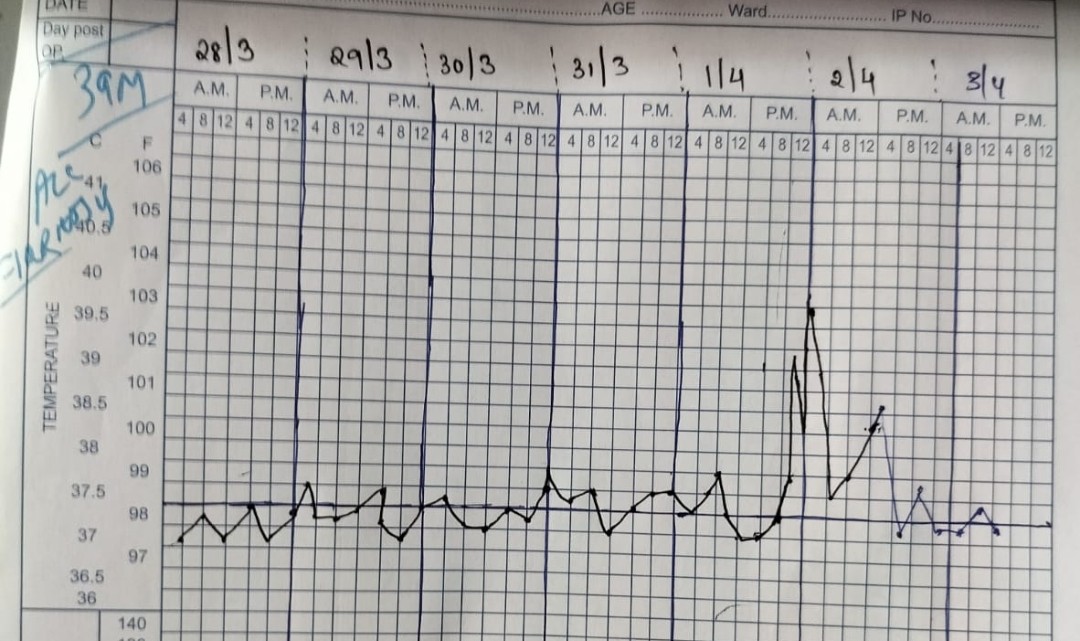
[03-04-2025 14.24] PPM 1: Fever spikes nil today. Yet to collect the ascitic fluid report to check if it was SBP!
EMR summary:
Age/Gender: 39 Years/Male
Address:
Discharge Type: Relieved
Admission Date: 28/03/2025 12:53 PM
Name of Treating Faculty
(AP) (PG3) (PG2) (PG1) (PG1)
Diagnosis
DECOMPENSATED CHRONIC LIVER DISEASE WITH ASCITES SECONDARY TO ALCOHOL ESOPHAGEAL VARICES (EV LIGATION DONE ON 07/05/2024)
UMBILICAL HERNIA
NO HEPATIC ENCEPHALOPATHY
Case History and Clinical Findings
PATIENT CAME WITH COMPLAINTS OF ABDOMINAL DISTENSION SINCE 2 YEARS.C/O SWELLING IN UMBILICAL REGION SINCE 9 MONTHS.
HOPI:PATIENT WAS APPARENTLY ASYMPTOMATIC 2 YEARS BACK THEN NOTICED DISTENSION OF ABDOMEN INSIDIOUS IN ONSET GRADUALLY PROGRESSIVE NO Aggravating OR RELEIVING FACTORS ASSOCIATED With SWELLING IN Umbilical REGION INSIDIOUS IN ONSE GRADUALLY PROGRESSIVE IN NATURE AGGREVATED ON COUGH NO RELIEVING FACTOR NOT ASOCIATED WITH PAIN.H/O BILATERAL PEDAL EDEMA EXTENDING UPTO KNEE INSIDIOUS IN ONSET PROGRESSIVE NO AGGREVATING OR RELIEVING FACTORS.H/O DECREASED URINE OUTPUT.NO H/O CONFUSION, HEMATURIA.NO H/O FACIAL PUFFINESS,FEVER,ABDOMINAL PAIN,NAUSEA,VOMITING,CONSTIPATION,LOOSE STOOLS,.NO H/O HEMATEMesIS,MELENA,DYSPHAGIA,CHEST PAIN,PND,ORTHOPNEA.
PAST HISTORY:K/C/O CHRONIC LIVERDISEASE SINCE 2 YEARS N/K/C/O T2DM/HTN/TB/EPILEPSY/THYROID/CVA/CAD
PAST MEDICAL HISTORY: 2 UNITS OF PRBC TRANSFUSION ON MAY 2024 OUTSIDE HOSPITAL
ESOPHAGEAL VARICES LIGATION ON 07/05/24 PERSONAL HISTORY:
MIXED DIET NORMAL APPETITE
BOWEL HABIT NORMAL
BLADDER DECREASED URINE OUTPUT ADEQUATE SLEEP
CHRONIC ALCOHOLIC SINCE 20 YEARS STOPPED 2 YEARS BACK CHRONIC SMOKER SINCE 20 YEARS STOPPED 2 YEARS BACK FAMILY HISTORY NOT SIGNIFICANT
GENERAL EXAMINATION PATIENT IS C/C/C
B/L PITTING PEDAL EDEMA EXTENDING TO KNEE PRESENT NO PALLOR NO ICTERUS NO LYMPHADENOPATHY NO CLUBBING
PR 94BPM
BP 110/70 MM OF HG RR 20CPM
SYSTEMIC EXAMINATION
CVS S1S2 HEARD NO MURMUR
RS BILATERAL AIR ENTRY PRESENT NVBS + CNS NFND
P/A :
INSPECTION : ABDOMEN DISTENDED UMBILICUS CENTRAL AND SWELLING OF UMBILICUS MEASURING 3X4CM WITH COUGH IMPULSE LIKELY UMBILICAL HERNIA.ALL QUADRANTS OF ABDOMEN MOVING ACCORDINGLY WITH RESPIRATION.
PALPATION: ABDOMEN SOFT NON TENDER.
PERCUSSION:DULL NOTE DETECTED OVER ENTIRE ABDOMEN D/T GROSS ASCITES.FLUID THRILL ELICITED.SHIFTING DULLNESS +
AUSCULTATION BOWEL SOUNDS HEARD.
SURGERY REFERRAL DONE I/V/O UMBILICAL HERNIA:
IMPRESSIVE : UMBILICAL HERNIA REPAIR ONCE PATIENT IS STABILISED. COURSE IN THE HOSPITAL:
39 YEARS OLD MALE CAME WITH ABOVE MENTIONED COMPLAINTS.NECCESSARY INVESTIGATIONS WERE DONE AND WAS DIAGNOSED AS DECOMPENSATED CHRONIC LIVER DISEASE SECONDARY TO ALCOHOL ,ESOPHAGEAL VARICES ,UMBILICAL HERNIA,NO ENCEPHALOPATHY WITH CHILD PUGH SCORE OF 8, MELD NA SCORE OF 8 MELD SCORE OF 11.TOTAL 4 DIAGNOSTIC AND THERAPEUTIC ASCITIC TAP WAS DONE AND ASCITIC FLUID WAS SENT FOR SAAG,AMYLASE,LIPASE,LDH,ALBUMIN,CELL COUNT
,CYTOLOGY.WEIGHT ON ADMISSION 70KGS AND ABDOMINAL GIRTH 104CMS.ON DISCAHRGE WEIGHT 62KGS AND ABDOMINAL GIRTH 94.5 CMS.H/O FEVER SPIKE AFTER 3RD ASCITIC TAP FOR WHICH INJ MONOCEF 2GM IV/BD WAS STARTED FOR TWO DAYS NO FEVER SPIKE LATER. PATIENT WAS TREATED CONSERVATIVELY AND HEMODYNAMICALLY STABLE HENCE BEING Discharged.
Investigation
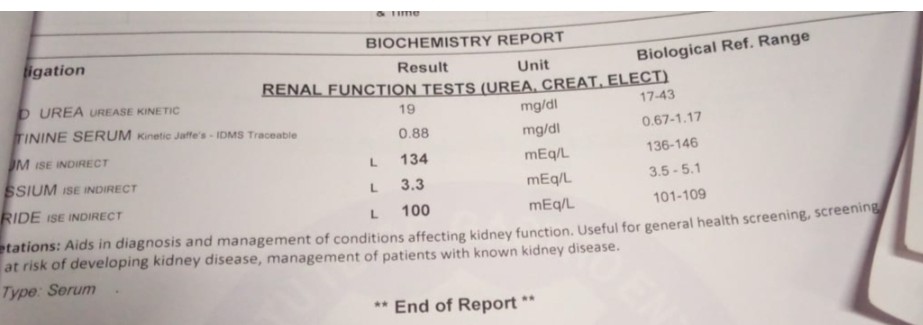
BLOOD UREA28-03-2025 03:14:PM14 mg/dl42-12 mg/dl SERUM CREATININE28-03-2025 03:14:PM0.8 mg/dl1.3-0.9 mg/dL SERUM ELECTROLYTES (Na, K, C l) 28-03-2025 03:14:PM SODIUM138 mmol/L145-136 mmol/LPOTASSIUM4.5 mmol/L5.1-3.5 mmol/LCHLORIDE106 mmol/L98-107 mmol/LLIVER FUNCTION TEST (LFT) 28-03-2025 03:14:PM Total Bilurubin1.81
mg/dl1-0 mg/dl Direct Bilurubin0.40 mg/dl0.2-0.0 mg/dl SGOT(AST)47 IU/L35-0 IU/LSGPT(ALT)31 IU/L
45-0 IU/L
ALKALINE PHOSPHATASE168 IU/L280-53 IU/L
TOTAL PROTEINS6.4 gm/dl8.3-6.4 gm/dlALBUMIN2.0 gm/dl5.2-3.5 gm/dlA/G RATIO0.45STOOL FOR OCCULT BLOOD29-03-2025 11:11:AM
Positive LIVER FUNCTION TEST (LFT) 30-03-2025 07:45:AM Total Bilurubin1.18 mg/dl1-0
mg/dl direct Bilurubin0.25 mg/dl0.2-0.0 mg/dl
SGOT(AST)36 IU/L
35-0 IU/L
SGPT(ALT)23 IU/L
45-0 IU/L
ALKALINE PHOSPHATASE135 IU/L280-53 IU/LTOTAL PROTEINS5.6 gm/dl8.3-6.4 gm/dlALBUMIN2.0 gm/dl5.2-3.5 gm/dl A/G RATIO0.44BLOOD UREA30-03-2025 07:45:AM12 mg/dl
42-12 mg/dl
SERUM CREATININE30-03-2025 07:45:AM0.8 mg/dl1.3-0.9 mg/dl
SERUM ELECTROLYTES (Na, K, C l) 30-03-2025 07:45:AM SODIUM137 mmol/L145-136
mmol/LPOTASSIUM3.5 mmol/L5.1-3.5 mmol/LCHLORIDE100 mmol/L98-107 mmol/L
SERUM ELECTROLYTES (Na, K, C l) 30-03-2025 12:04:PM SODIUM136 mmol/L145-136
mmol/LPOTASSIUM3.7 mmol/L5.1-3.5 mmol/LCHLORIDE101 mmol/L98-107 mmol/L
BLOOD UREA30-03-2025 10:28:PM16 mg/dl42-12 mg/dl
SERUM CREATININE30-03-2025 10:29:PM0.7 mg/dl1.3-0.9 mg/dl SERUM ELECTROLYTES (Na, K, C l) 30-03-2025 10:29:PM SODIUM139
mmol/L145-136 mmol/LPOTASSIUM3.8 mmol/L5.1-3.5 mmol/LCHLORIDE103 mmol/L98-107 mmol/LLIVER FUNCTION TEST (LFT) 30-03-2025 10:29:PM Total Bilurubin1.01 mg/dl1-0 mg/dlDirect Bilurubin0.20 mg/dl0.2-0.0 mg/dl SGOT(AST)43 IU/L35-0 IU/LSGPT(ALT)26 IU/L45-0 IU/LALKALINE PHOSPHATASE152 IU/L280-53 IU/LTOTAL PROTEINS6.1 gm/dl8.3-6.4 gm/dlALBUMIN2.0 gm/dl5.2-3.5 gm/dl A/G RATIO0.49SERUM ELECTROLYTES (Na, K, C l) 01-04- 2025 11:48:PM SODIUM136 mmol/L145-136 mmol/LPOTASSIUM4.2 mmol/L5.1-3.5 mmol/LCHLORIDE100 mmol/L98-107 mmol/LBLOOD UREA01-04-2025 11:48:PM20 mg/dl42-12
mg/dl SERUM CREATININE01-04-2025 11:48:PM0.9 mg/dl1.3-0.9 mg/dl HEMOGRAM ON 28/3/25
HAEMOGLOBIN 7.7 gm/dl TOTAL COUNT 3,400 cells/cumm NEUTROPHILS 53 % LYMPHOCYTES 33 % EOSINOPHILS 06 % MONOCYTES 08 % BASOPHILS 00 % PCV 23.2 vol % M C V 77.9 fl M C H 25.8 pg M C H C 33.2 % RDW-CV 18.1 % RDW-SD 51.7 fl RBC COUNT 2.98
millions/cumm PLATELET COUNT 1.2 lakhs/cu.mm RBC predominently Normocytic, normochromic with few macrocytes, microcytes torget cellsWBC In adeqaute PLATELETS Adeqaute HEMOPARASITES No hemoparasites seen IMPRESSION bicytophenia.
HEMOGRAM ON 30//3/25
HAEMOGLOBIN 7.5 gm/dl TOTAL COUNT 3,000 cells/cumm NEUTROPHILS 47 % LYMPHOCYTES 37 % EOSINOPHILS 06 % MONOCYTES 10 % BASOPHILS 00 % PCV 22.2 vol % M C V 77.6 fl M C H 26.2 pg M C H C 33.8 %RDW-CV 17.6 % RDW-SD 50.5 fl RBC COUNT 2.86
millions/cumm PLATELET COUNT 1.16 lakhs/cu.mmRBC predominently Normocyticnormochromic with few macrocytesmicrocytes torget cellsLight MicroscopyWBC Decreased on smear PLATELETS In Adequate HEMOPARASITES No hemoparasites seen IMPRESSION Bicytophenia
HEMOGRAM ON 31/3/25
HAEMOGLOBIN 7.5 gm/dl TOTAL COUNT 3,000 cells/cumm NEUTROPHILS 47 % LYMPHOCYTES 37 %EOSINOPHILS 06 %MONOCYTES 10 % BASOPHILS 00 %PCV 22.2 vol % M C V 77.6 fl M C H 26.2 pg M C H C 33.8 % RDW-CV 17.6 % RDW-SD 50.5 fl RBC COUNT 2.86
millions/cummPLATELET COUNT 1.16 lakhs/cu.mm RBC predominently Normocyticnormochromic with few macrocytesmicrocytes torget cellsLight MicroscopyWBC Decreased on smear Light MicroscopyPLATELETS In Adeqaute Light MicroscopyHEMOPARASITES No hemoparasites seen Light MicroscopyIMPRESSION Bicytophenia
HEMOGRAM ON 01/4/25
HAEMOGLOBIN 8.0 gm/dl TOTAL COUNT 3,300 cells/cumm NEUTROPHILS 40 %LYMPHOCYTES 40 % EOSINOPHILS 10 % MONOCYTES 10 % BASOPHILS 00 % PCV 23.5 vol %M C V 76.5 fl M C H 26.1 pg M C H C 34.0 % RDW-CV 17.7 % RDW-SD 50.4 fl RBC COUNT 3.06 millions/cumm
PLATELET COUNT 92,000 lakhs/cu.mm RBC Normocytic normochromic with fewmicrocytesWBC Decreased counts on smear PLATELETS In AdeqauteHEMOPARASITES No hemoparasites seenIMPRESSION pancytopenia
HEMOGRAM 03/4/25
HAEMOGLOBIN 7.8 gm/dl TOTAL COUNT 2,400 cells/cumm NEUTROPHILS 64 % LYMPHOCYTES 21 % EOSINOPHILS 05 % MONOCYTES 10 % BASOPHILS 00 % PCV 23.4 vol % M C V 78.0 fl M C H 26.0 pg M C H C 33.3 % RDW-CV 18.1 % RDW-SD 52.6 flRBC COUNT 3.00
millions/cummPLATELET COUNT 72,000 lakhs/cu.mm RBC Normocytic normochromic with fewmicrocytes WBC decreased counts on smear PLATELETS Inadequate HEMOPARASITES No hemoparasites seen IMPRESSION pancytopenia
28/3/25: INR 1.11 APT 32SEC PT 16 SEC BT 2 MIN CT 4 MIN SR LDH 350
28/3/25 ASCITIC FLUID ANALYSIS :
PROTIEN 0.9 SUGAR 101 AMYLASE 202 LDH 130.8 ALBUMIN 0.37 SAAG 1.63 CELLS NIL CLEAR PALE YELLOW
ASCITIC FLUID CYTOLOGY ON 2/4/25 SCANT CELLULAR CYTOSMEAR SHOWS MESOTHELIAL CELLS FEW REACTIVE MESOTHELIAL CELLS AND LYMPHOCYTES.NO EVIDENCE OF ATYPICAL CELLS IN SMEAR STUDIED.
USG ABDOMEN ON 28/3/25
CIRRHOSIS OF LIVER WITH PORTAL HTN,UMBILICAL HERNIA 19 MM DEFECT,GROSS ASCITES,SPLENOMEGALY.
Treatment Given(Enter only Generic Name)
1. FLUID RESTRICTION <1.5 L/DAY
2. SALT RESTRICTED DIET <2GM/DAY
3. TAB FUROSEMIDE 40MG PO/OD
4. TAB ALDACTONE 100MG PO/OD
5. TAB PROPRANOLOL 20MG PO/BD
6. HEPATIC PROTIEN POWDER 2 SCOOPS IN 200 ML MILK
7. 3 EGG WHITE PER DAY
8. WEIGHT AND ABDOMINAL GIRTH MONITORING
9. SYP LACTULOSE 15ML/TID
Advice at Discharge
1. FLUID RESTRICTION <1.5 L/DAY TO BE CONTINUED
2. SALT RESTRICTED DIET <2GM/DAY TO BE CONTINUED
3. TAB ALDACTONE 100MG PO/OD X2 WEEKS
4. TAB PROPRANOLOL 20MG PO/BD X2WEEKS
5. HEPATIC PROTIEN POWDER 2 SCOOPS IN 200 ML MILK X2WEEKS
6. 3 EGG WHITE PER DAY TO BE CONTINUED
7. SYP LACTULOSE 15ML/TID X 1 WEEK
Follow Up
REVIEW TO GENERAL MEDICINE OPD AFTER 2 WEEKS /SOS REVIEW TO GENERAL SURGERY OPD AFTER 2 WEEKS /SOS
When to Obtain Urgent Care
IN CASE OF ANY EMERGENCY IMMEDIATELY CONTACT YOUR CONSULTANT DOCTOR OR ATTEND EMERGENCY DEPARTMENT.
Preventive Care
AVOID SELF MEDICATION WITHOUT DOCTORS ADVICE, DONOT MISS MEDICATIONS. In case
of Emergency or to speak to your treating FACULTY or For Appointments, Please Contact: For Treatment Enquiries Patient/Attendent Declaration : - The medicines prescribed and the advice regarding preventive aspects of care, when and how to obtain urgent care have been explained to me in my own language
SIGNATURE OF PATIENT /ATTENDER
SIGNATURE OF PG/INTERNEE
SIGNATURE OF ADMINISTRATOR
SIGNATURE OF FACULTY
Discharge Date Date:07/04/25 Ward:MMW Unit:4
[08-04-2025 16:55] PA: Sar ji medicine ghulo diyechen paoya jacche na
[08-04-2025 16:55] PA: Onno kampani achaa
[08-04-2025 16:55] PA: Ki korbo
[08-04-2025 17:04] PPM 1: Onno Kompany niye chobi share korun
[08-04-2025 20.12] PA: LACTULOSE ORAL SOLUTION, PRONOL 10
[08-04-2025 21:35] PPM 1: Thik achhe.

[15-04-2025 19:17] PPM 1: Kone side ta?
[16-04-2025 00:44] PA: Dan side
[16-04-2025 06:13] PPM 1: Patient ki daan side a beshi shuye thaken?
[16-04-2025 21:02] PA: Haa

Ar ekhono weight 60kg royeche
[23-04-2025 17:01] PPM 1: Uni Bortoman medicine ki khacchen tar packet er chobi tule share korun jaate dose tao dekha jai


[23-04-2025 19.46] PA: Sir pha fula ta komche
Kintu navi fula ta kome ni sir
[23-04-2025 21:19] PPM 1: Otao kombe
[27-04-2025 16:03] PA: Sir হজম শক্তি টা কম হচ্ছে। আর খাওয়ার রুচি দুই দিন ধরে নেই
[27-04-2025 19:03] PPM 1: Roj haatha chola koto ta korchen?
[27-04-2025 19:17] PA: Haatha chola aektu kom kore
[27-04-2025 19:19] PPM 1: Aaste aaste barano dorkar
[09-05-2025 21:57] PA: Sir bollam পেট আর পা Abar fulche
[09-05-2025 21:58] PA: Ki korbo
[09-05-2025 21:59] PA: Akhane to ar jol bar kora hoy nai
[10-05-2025 06:44] PPM 1: Chobi pathan jate patient er mukh na dekha jai

[10-05-2025 21.01] PPM 1: Oshudh ki maajhe bondho chilo? Bortoman oshudh gunor chobi share korun
[10-05-2025 23.02] PA: Oshudh Bondho to hoy na.




[11-05-2025 09:42] PPM 1: Ekta oshudh bondho hoyechilo tai abar fuleche.
Abar ota shuru korte habe. Tablet Lasix 40 mg sokale ekbar ek soptaaho
[11-05-2025 10:57] PA: Sir পেছাপ kom hoy
[11-05-2025 10:58] PPM 1: Aei oshudh ta khele pecchap beshi habe
[11-05-2025 10:58] PPM 1: Roj patient er ojon kore janaben
[11-05-2025 12:40] PA: Oshudh ta ki vabe khabe
[11-05-2025 13:00] PPM 1: Sokale ekta tablet joler saathe. Aer aageo uni khacchilen
[11-05-2025 13:15] PA: Na aage খাওয়ানো hoy nai
[11-05-2025 13:40] PPM 1: Hoyechilo. Amar mone achhe. Oshudh ta dekhe bojha mushkil. Otar ashol naam holo frusemide. 40 mg sokale ekbar
[12-05-2025 09:45] PA: Sir bollam navi ta aro aktu fulche
Aro Baitha hoyche
[12-05-2025 16:30] PPM 1: Oshudh ta kaaj korte soptaho khanik lagbe kintu nabhi te byatha mane hothath kore nabhi ta feteo jete pare tai kacher health center er daktar ke oti oboshyoi dekhiye neben shiggiri
[12-05-2025 16:32] PPM 1: 👆dekheo mone hocche jeno ektu kaalche hoye geche kajei fete jawar sombhobona royeche tai shiggiri okhane local daktar ke dekhiye neben.
[12-05-2025 18:19] PA: Sir apner okhane abar ki jabo
[12-05-2025 18:36] PPM 1: Aage local government health center a ekbar dekhiye nin.
[16-05-2025 18.24] PA: Sir bollam navi ta diye blood ber hoy.
[16-05-2025 21:34] PPM 1: Local government health center a ekbar dekhiye nin
[17-05-2025 17:22] PA: Sir bollam doctor ke dakhi lam
doctor bollo jol thakle surgery Kora Jabe na.
[17-05-2025 17:25] PA: 1L jol bar kora hoyeche
Are wait 55kg.


[17-05-2025 18.16] PPM 1: Aekhon asha kori patient ektu aaram peyechen?
[17-05-2025 19:01] PA: Ha
[17-05-2025 19:07] PA: Kintu navi ta, Suye thakle navi bose jai, Ar daraile tan pore.
[17-05-2025 19:13] PPM 1: Okhane chap diye dhore rakhle ki taan ta kome?
[17-05-2025 19:58] PA: Belt Diye
Chaap Diye rakhle to Baitha kore na.
Kintu belt na porle taan taan pore baitha kore
[17-05-2025 20:08] PA: Ar belt porle fosa pore
[17-05-2025 20:13] PPM 1: Just haath diye chepe rakhben.
[20-05-2025 16:45] PA: Sir bollam jol ta sukaite koto din lagbe.
[20-05-2025 16:58] PPM 1: Aajker ojon koto?
Shorirer jol aekhon kemon ache chobi pathaben jaate patient ke chena na jai

[20-05-2025 19:16] PPM 1: Pa aer chobi tao share korben

[20-05-2025 19:41] PPM 1: Oh anek komeche!
[20-05-2025 19:51] PA: Navi ta ki akhon surgery kora jabe
[20-05-2025 19:56] PPM 1: Surgeon er upor sheta nirbhor korche
[20-05-2025 20:04] PA: Sir tahole Apnar okhane Jabo na nki.
[20-05-2025 20:06] PPM 1: Patient ekhane operation korate chaichen? Jol ta komle nabhir somosya tao kome jaabe asha korchi ebong operation koranor dorkar nao hote pare. Operation korano ta ektu risky hoye jete pare
[10-06-2025 11:13] PA: Sir bollam navi ta kom tache na
[10-06-2025 11:16] PA: Navi tare akhon bese samosa
[10-06-2025 15:21] PPM 1: Navi tar aekhon ki somosya?
[10-06-2025 15:32] PA: Navi ta fula komena
[10-06-2025 15:35] PA: Ar Navi theke Aata aata Ras Bar hay
[11-06-2025 15.37] PA: 


[22-06-2025 07.01] PPM 1: Hain okhankar medicine ta continue korun ebong apnar patient er peter ebong payer fola kemon shetar chobi roj share korun

[22-06-2025 11.20] PPM 1: 👍
 [24-06-2025 18:15] PA: Sir abar pet ta fule গেলো kano
[24-06-2025 18:15] PA: Sir abar pet ta fule গেলো kano
 [30-06-2025 17.42] PA:
[30-06-2025 17.42] PA: 


[11-06-2025 16:14] PPM 1: Eta operation kora dorkar shiggiri!
[11-06-2025 16:18] PA: To apnar okane ki Jabo
[11-06-2025 16:35] PPM 1: Hain okhane kacha kachi government hospital a hoye gele apnar hoito subidhe hoto
[11-06-2025 17:02] PA: Kintu Akhenea to dekheiche, Jol thale operation kora jabe na Bolche
[11-06-2025 17:06] PPM 1: Ta oboshyo sob jaigai asubidhe habe korte. Ektu risky o habe. @PPM3 your inputs on the feasibility of operating this umbilical hernia before it ruptures and all his ascites comes out in one go?
[11-06-2025 17.49] PPM 3: The problem is real. Even our surgeons hesitate in CTP C cirrhosis. But it has to be operated. No other way.
[21-06-2025 18:02] PA: Bollam sir
Navi ta surgery Kora hoyeche
[21-06-2025 18:04] PA: Ar bollam
Apner medicine tei cholbe naki
[21-06-2025 18:12] PPM 1: Khub bhalo. Kothai?
[21-06-2025 18:13] PPM 1: Notun nabhir ekta chobi pathan

[21-06-2025 18:24] PPM 1: 👍Oi kata jaigatar chobi? Notun nabhir chobi
[21-06-2025 18:24] PA: Bandage kora acha
[21-06-2025 18:25] PPM 1: Kothai koralen?
[21-06-2025 18:28] PA: Coochbehar Nursing home
[21-06-2025 18:29] PPM 1: Koto khoroch holo?
[21-06-2025 18:32] PA: 80 হাজার
[21-06-2025 18:39] PPM 1: 👆@30F PA what would you think about this cost? What can be done so that these operations can be done in the district hospitals free of cost?
[21-06-2025 220.08] 30F PA: Sir,
In the current socio-political Indian scenario, free of cost treatment is possible in the govt. Hospitals. However, the general people face the following obstructions -
1. The so called agents (Dalal Chokro) of the Hospitals with whom the whole system is synced. Doctors, nurses and so on. They promise the people to get the thing done, however, demand money on this behalf. This is the core of the corruption belt at the grassroot level.
2. Lack of infrastructure at the district hospitals and Referring Culture. Whenever, they get any critical case, the local hospitals refer it to some bigger cities like Siliguri. It becomes impossible for the people living in the remote areas to go to bugger cities and get their treatment done.
3. If you ask this patient, majority of the operations are done in the private nursing homes by the Doctors who are working at the Govt. Hospitals. They have daily shifts over in the Govt. Hospitals and night shifts in the private hospitals. Majority of them see patients in government OPDs and refer them to the respective Private Clinics with which they have tie up with. This is the second and most dangerous tier when people get trapped. Now many doctors will give many excuses, but as a legal academician I am consciously using the term ENTRAPMENT. The people become helpless and they become bound to spend money in these so called private hospitals and get their things done.
[21-06-2025 20:14] 30F PA: Now coming to your question what can be done ?
1. At the very district levels, better infrastructure should be built up on which the Doctors can be more humane to the health issues of the people.
2. The number of the medical professionals should be increased at the govt. Aided institutions.
3. The exhaustive working hours of the Doctors should be reduced to a reasonable hour so that they can also act like humanes.
4. The overall mentality of the Medical professions should not be seen as an investment. It should be considered as the most noble profession where the most passionate students are coming in.
Whereas in this current Socio-economic backdrop, people take medical courses as Investment. During the 4 to 6 years course if I am expending 6 crore rupees ( the value should be counted on the basis of both physical, mental and economic measures) then from this profession atleast 12 crore ( means double or more) amount has to be recovered. Whenever this mentality ushers in, there comes desaster.
[21-06-2025 20:16] 30F PA: Both the Doctors as well as the general people have issues with the system. The system should be changed or you have to be a better resourceful person in order to get your job done in any government institution of the country.
[21-06-2025 20:22] PA: Sir
Akhene je surgery koreyeche
Akhene medicine diyeche
AKhankar medicine tao cholbe naki.
[21-06-2025 20:22] PPM 3: It is not free of cost Sir. Someone has to pay the bill, in this case, the taxpayer. I was wondering whether schemes like Ayushman Bharat (or similar state specific insurance schemes) can help patients get treatment upto a predefined threshold free of charge at even empanelled private facilities?
[21-06-2025 20:27] PPM 3: Also, all treatment in all tiers of health facilities is free of cost to the patient in WB, even upto biologicals used in rheumatology.
The problem in this specific case might be whether the district hospital has enough capability to operate on a decompensated cirrhotic patient? In all likelihood they would be referring to a tertiary medical college, where again the treatment is free but getting a date for a surgery becomes a problem, because of the enormous wait-list.
[21-06-2025 20:53] PPM 1: Okhane ki medicine diyeche share korben

[22-06-2025 07.01] PPM 1: Hain okhankar medicine ta continue korun ebong apnar patient er peter ebong payer fola kemon shetar chobi roj share korun


[22-06-2025 11.20] PPM 1: 👍

[23-06-2025 12:48] PPM 1: 👍Darano jacche?
[23-06-2025 15:39] PA: Jacche kintu.
[23-06-2025 15:39] PA: Patient sob somoy, oster oster kore
[23-06-2025 16.40] PPM 1: Dariye side theke chobi tulte parle bhalo hoi.[24-06-2025 20:12] PPM 1: Liver er somosya ta to aekhono puro puri jaini
[24-06-2025 20:12] PPM 1: Pa folar ekta chobi pathaben
PPM 1: 👍
[25-06-2025 11:26] PA: Pechap ta kom hoche
[25-06-2025 11:27] PA: ওষুধ টা Din ne 2bar khayo jabe (FRUSEMIDE TABLET LASIX 40mg)
[25-06-2025 13:03] PPM 1: Pechchap ta 24 ghonta sokal 8:00 theke porer din sokal 8:00 obdhi erokom ekta container a 👇
Mepe janaben
Aeki bhabe jol shedin sokal 8:00 theke porer din sokal 8:00 ta obdhi koto kheyechen shetao mepe janaben
[27-06-2025 14:56] PPM 3: https://www.journal-of-hepatology.eu/article/S0168-8278(25)00235-1/fulltext
[27-06-2025 14:57] PPM 3: @PPM1Sir The recent (May 2025) EASL Guideline on extrahepatic abdominal surgery in patients with cirrhosis
[27-06-2025 14:57] PPM 3: With/without decompensation
[27-06-2025 14:58] PPM 3: Recommendations
•
Surgery for symptomatic hernia may be considered in experienced centres after careful risk assessment (LoE 3, strong recommendation, strong consensus).
•
Elective surgery in experienced centres should be preferred, as emergency surgery for symptomatic hernia is associated with worse outcomes (LoE 3, strong recommendation, strong consensus).
[27-06-2025 15:01] PPM 3: Details: (Quoted verbatim from the EASL CPG, for references see the full text)
Morbidity following elective umbilical hernia repair varies between 7% and 20%, with reported mortality rates ranging from 0% to 5.5%. Due to the heightened risk in decompensated cirrhosis, some advocate for non-surgical management. However, a prospective observational study found that conservative treatment or a "wait-and-see" approach was associated with higher mortality, likely due to an increased risk of incarceration. Emergency umbilical hernia repair, particularly in cases of incarceration, carries significantly higher complication rates and up to a 7-fold increase in mortality compared to elective surgery. Consequently, a "fix it while you can" strategy has been proposed for patients with cirrhosis with umbilical hernias. Poor surgical outcomes are associated with MELD scores >15, CTP class C, poorly controlled ascites, symptomatic hernias, and emergent presentations. Moreover, uncontrolled ascites significantly increases the risk of hernia recurrence (relative risk 8.51) and impairs wound healing. Thus, preoperative measures to manage portal hypertension and ascites, such as transjugular intrahepatic portosystemic shunt (TIPS) placement, may be considered. In addition, mesh repair is preferred over suture repair, as it significantly reduces the risk of recurrence (2.7% vs. 14.2%).
[27-06-2025 19:44] PPM 1: 👏
[28-06-2025 11:18] PA: Pechchap 24 gontay 1.5 L. And jol 24 gontay kachhe 2 L.
[28-06-2025 12:52] PPM 1: Uni oshudh ki khacchen?
[28-06-2025 12:53] PPM 1: 1.5 litres to kom pecchap noi

[29-06-2025 19:23] PA: Sir পেট fula ta komtache na
[29-06-2025 19:27] PPM 1: 👆aei oshudh ta kobar khacchen?
[29-06-2025 19:30] PA: Sokale kore 1 bar khacche
[29-06-2025 19:33] PPM 1: Duto tablet nite paren kichu din
[29-06-2025 19:33] PPM 1: Kintu duto tablet newa kalin roj payer ebong peter folar chobi share korben


[03-07-2025 09.36] PA: Sir sheelai ta diye jol bar hoy
[03-07-2025 09:37] PA: Ar kichu Khele acid Hoi Jaye
[03-07-2025 09:43] PA: Dine dine patient to aaro kharab hoy যাচ্ছে
[03-07-2025 14:24] PPM 1: Abar pet theke kichu jol baar kore dewa proyojon
[10-07-2025 16:17] PA: Sir patient ke to bachite parlam na 🥲
[10-07-2025 16:21] PPM 1: Sheki!
[10-07-2025 16:22] PA: Kalke 5ta
[10-07-2025 16:23] PPM 1: Hothath? Hospital a niye jawa hoyechilo?
[10-07-2025 16:24] PA: Ha
[10-07-2025 16:26] PPM 1: Aekhon unar barite unar stree achen? Are unar bacchder boyesh koto?
[10-07-2025 16:27]PA: 17
[10-07-2025 16:32] PA: আর এক ছেলে আছে 15 বয়স
[10-07-2025 16:35] PPM 1: Accha. Orai aekhon unar Streer shohai hoye darabe. Asha korchi unara shobai abar bhalo bhabe thakte parben
No comments:
Post a Comment