
THIS IS AN ONLINE E LOG BOOK TO DISCUSS OUR PATIENT'S DE-IDENTIFIED HEALTH DATA SHARED AFTER TAKING HIS SIGNED INFORMED CONSENT. HERE WE DISCUSS OUR PATIENT'S PROBLEMS THROUGH SERIES OF INPUTS FROM AVAILABLE GLOBAL ONLINE COMMUNITY EXPERTS WITH AN AIM TO SOLVE THOSE PATIENT'S CLINICAL PROBLEMS WITH COLLECTIVE CURRENT BEST EVIDENCE BASED INPUTS.
This is the case of a 55 yr old male who is suffering with neck pain since May 2024. By profession he had to ride bike daily for 1-2 hrs which aggravated his shoulder pain and had relief only when he lied on the bed. Day by day his pain increased and developed a stiff neck.
He used a cervical pillow and neck collar advised by a local physician. He found relief more when laying on bed. Slowly after 2-3 months he felt better.
Now again the patient is suffering with neck pain and uneasiness to move the neck freely. He is feeling imbalance while walking and pressure on his knees. At present the patient is under the medication of Blood pressure and cholesterol.

PA - Hatur ei point ekta pain hoy ja hatachola korle bare r siri othanama korte bises kore namer somoy
balance harie jay .sue thakle relief pay.
Translation - "There's a point in the knee where pain occurs, which increases when walking and
especially when going up and down stairs, particularly when coming down. Balance is lost during this.
There's relief when lying down."


[05-03-2025 08:07] PPM 1: Hater majher angul fold korte bes lagche ..
[05-03-2025 08:07] PPM 1: Ki korbe pl bolun..jodi kono test korte hoy bolben..
[05-03-2025 08:07] PA: Bes kichudin holo
[05-03-2025 08:07] PA: R gharer problem ta last June theke
[05-03-2025 08:07] PA: Oi somoy pray 15 days bed ridden chilo ,marattok kosto peyechilo
[05-03-2025 08:07] PA: Gharer collar r ekta spondylitis pillow use kore komechilo.orthopedic
dekhiechilen
[05-03-2025 08:07] PA: Pressure, cholesterol medicine khay r dry eye problems.
[05-03-2025 08:07] PA: Kajer jonno bike chalay khub
[05-03-2025 08:07] PA: Pither diker Reeb box r kache khub lagche .phone besikhon dhore rakhte
parchena
[05-03-2025 08:07] PA: Pressure r cholesterol medicine khay
"It's quite painful to fold the middle finger of the hand. Please tell me what to do, and if any tests are
needed, let me know. It's been a few days. The back problem has been there since last June. At that
time, I was bedridden for about 15 days and experienced severe pain. Using a collar and a spondylitis
pillow helped reduce it. I consulted an orthopedic doctor. I take medicine for blood pressure and
cholesterol and have dry eye problems. I ride a bike a lot for work. There's a lot of pain near the rib box
at the back. I can't hold the phone for long. I take medicine for blood pressure and cholesterol."



[05-03-2025 14:52] PA: He used cervical pillow and neck collar as per doctor's advise and almost bed ridden for 2-3months. after he feels better and back in his normal activities.
[05-03-2025 15:03] PA: Now he feels again' neck pain and uneasiness to movement.Even he feels unstable when he steps ...
[05-03-2025 15:05] PA: He also feels that his knee twist when he walks.
[05-03-2025 15:06] PA: Now he takes cholesterol nd blood pressure medicine.
[05-03-2025 15:07] PA: What should he do pl suggest him
[05-03-2025 15:15] PPM 1: We need to see these films
Didn't we do any X-rays when he came here in our hospital?
[05-03-2025 15:16] PPM 1: To begin with, please add his immediate advocate here and ask him to share
his daily food plates and hourly activities
[05-03-2025 15:26] PA: No.
PA - Dinner at 10.09pm with rice aloo curry and pickle.
PPM 1 - 👍
[06-03-2025 06:56] PPM 1: Please do also mention the patient's hourly activities.
[06-03-2025 07:00] PA: He wakes up in the morning at 8 'O'clock then he takes a glass of hot
water. After freshening up he takes a cup of black tea with a thin arraroot or Marry biscuits.
[06-03-2025 07:03] PA: 8.30Am -He walks in his balcony or roof top and do light stretching exercises.
[06-03-2025 07:05] PA: Then he lies down on the bed for few minutes and after that he takes mobile or
read newspaper.
[06-03-2025 07:19] PPM 1: Did he feel any pain today or yesterday during the stretching exercises?
[06-03-2025 07:23] PA: Yes, little pain and confused that now he has to continue or stop for few days?
[06-03-2025 07:28] PA: After 9.15 he goes to bath and washes his everyday clothes. Then he carries
them up to the 3rd floor. Almost twice a week, he fills a bucket and washes with soap and even the
bedsheets, pillow covers,etc.,have to carry to the 3rd floor with that heavy bucket. After doing this he
feels tired.
[06-03-2025 07:28] PPM 1: Where and when exactly does he feel the pain during stretching? Can he
share a deidentified video of his stretching exercises and point to when and where does he feel the
pain?
[06-03-2025 07:29] PA: Ok, will share after few hours.
PPM 1 - Check out the deidentified video posted by one of our other patients here👇
[06-03-2025 07:31] PPM 1: That sounds like tiring work and should keep him physically fit. I also
gather he doesn't feel pain during that work.
[06-03-2025 07:35] PA: He is a very hard working man.
[06-03-2025 07:54] PPM 1: Would be interested to know how he became bedridden once earlier.
[06-03-2025 07:55] PA: Sharing his daily routine
[06-03-2025 07:56] PPM 1: Yes
Also need to know the details of these events👇
[05-03-2025 08:07] PA: Bes kichudin holo
[05-03-2025 08:07] PA: R gharer problem ta last June theke
[05-03-2025 08:07] PA: Oi somoy pray 15 days bed ridden chilo ,marattok kosto peyechilo
[06-03-2025 07:56] PA: Yes
[06-03-2025 08:02] PA: At the end of April he felt neck pain, stiffness, leg calf muscle cramps,
abdomen problems like uneasiness, indigestion, bloating, constipation etc several times. He is good
human being but very short tempered with very loud voice ...
[06-03-2025 08:04] PA: Sorry, it is by the end of Feb 24
[06-03-2025 08:07] PA: But end of March he looks like very tired, it was starting of summer, very hot
weather.
[06-03-2025 08:07] PPM 1: Was he absolutely alright before that?
[06-03-2025 08:08] PA: Although he continues his daily work.
[06-03-2025 08:10] PA: Almost but he has a chronic anxiety problem and appetite problem throughout
the year. but that time he has no neck pain.
[06-03-2025 08:11] PA: His morning Tea
[06-03-2025 08:11] PA: Without sugar
[06-03-2025 08:17] PA: By the end of April his pains were increasing in different parts like
neck, back side, knee, at several times it was really irritating for him.
[06-03-2025 08:21] PA: Few days after that he was unable to do his daily work and
became bedridden due to stiffness of neck with severe pain.
[06-03-2025 08:24] PA: 1st week of May he lost his father and it
was a great loss to his family and then he was very upset.
[06-03-2025 09:00] PA: Oh! Sorry it was 9 th June he lost his father permanently. Few days after that
in his area someone organised a meditation workshop for 5days and luckily, he
attended this program and it was very effective for him from pain and stressed life.
[06-03-2025 09:23] PA: Then he practices Sudarshan kriya and meditation. At 10 am he eats rice with
boiled potato or curry. After that, he takes some rest and goes out on a bike for his work. Between
12.30 to 1pm he has black tea fried chola. Then at 2 pm he returns home and uses the toilet for second
time, and from 2.30 to 3pm he has lunch. Afterwards lies down on the bed, takes rest, spends time on
his mobile and listens to songs. At 5.30 pm,if there is any work, he goes out again and then has one
cup of black tea. If needed, he even rides his bike for 1-2hours .after that between 7.30 to 8 pm he has a
light snack with little puffed rice. Then at 9.30 he returns home, freshen up, and at 10 he has
dinner. After one and half hours, he drinks water and then watches Tv until about 11.30pm. Then, from around 12.30, he uses his mobile before going to sleep. Between lunch and dinner, he smokes one
cigarette or bidi otherwise he can't sleep or his energy drops. and he ends up getting a cold. He smokes
3-4times. At night, if he takes a long time to fall asleep or don't get deep sleep he has to use toilet 2-
3times.
[06-03-2025 09:28] PA: Now he suffers mouth sores (which called slesha gha due to deficiency of vit c)
on both sides of his tongue.
[06-03-2025 09:29] PA: He takes cholesterol and blood pressure medicine daily
[06-03-2025 09:32] PA: Last month he tested urine routine test for time taking urination and 2_3times
he has to urinate at night. or day during when he takes short rest.
[06-03-2025 09:32] PA: It was normal.
[06-03-2025 10:30] PPM 1: Please share his cholesterol medication image here.
That could be an important reason for his current symptoms.
If he has never had any heart attack or brain attack then that medicine may be stopped after confirming
with the local doctor who prescribed it



PA - Cholesterol and blood pressure medicine takes as per doctor's advice in 2023. After that he didn't
go for further but medications and continuing the above medicines.






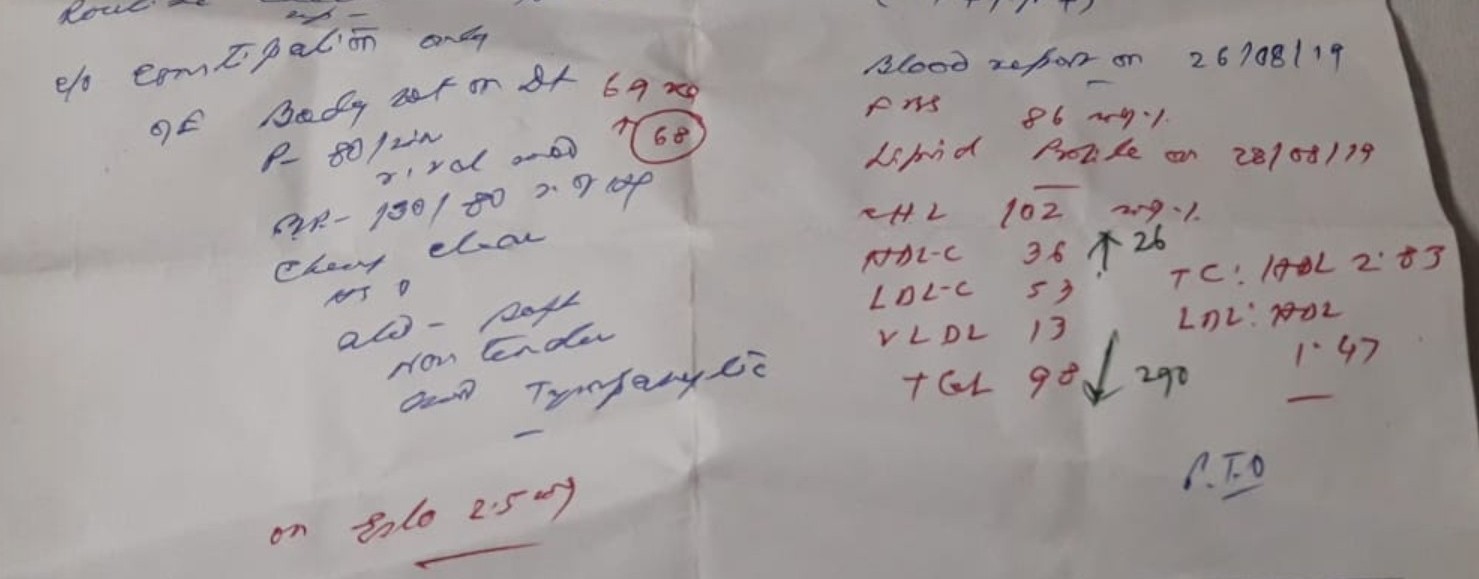
[06-03-2025 12:28] PA: This is 21/9/24 dated blood reports, after one year taking those medicines.
[06-03-2025 12:30] PA: Pl tell me what should he do or need to do any test?
[06-03-2025 12:32] PA: Today he woke up at 8am. Then hehad a glass of warm water.
[06-03-2025 12:33] PA: After freshening up he took cup of tea and biscuit at 8.30am
[06-03-2025 13:02] PA: The patient had black tea and nuts.
[06-03-2025 14:46] PA: The patient completed his lunch with rice and curries.
[06-03-2025 15:44] PA: After lunch the patient takes some rest and listening songs.
[06-03-2025 16:41] PPM 1: Serial lipid profile report?
[06-03-2025 16:42] PPM 1: 👆Date?
When was the first lipid profile done?
[06-03-2025 16:43] PPM 1: 👆this tablet rosumep 5/160 can be stopped. It could be one of the possible
reasons for his symptoms
[06-03-2025 16:44] PA: All reports are 21/09/24 dated.
[06-03-2025 16:47] PA: Should he check once again before withdrawal?
[06-03-2025 16:57] PPM 1: Can.
[06-03-2025 16:57] PPM 1: Try sharing the profile that made his doctor start him on the
rosuvastatin and fibrate medicine
[06-03-2025 16:58] PA: Pl write down the patient for which test is needed
[06-03-2025 16:59] PA: Ok
[06-03-2025 17:00] PPM 1: Serum fasting lipid profile
[06-03-2025 17:00] PA: This is
[06-03-2025 17:01] PPM 1: 👆 need to see that lipid profile after which he was started on
the medicine
[06-03-2025 17:04] PA: After 1 year of starting rosumep.
[06-03-2025 17:05] PA: Rosumep
[06-03-2025 17:08] PA: When he started 1st time TG was 285 and after 1 year taking
rosumep it is 81(5 months ago)



[06-03-2025 1816] PA - In 2018 he started cholesterol medicine.

[06-03-2025 21:38] PA: Patient had dinner at 9.30pm.
[06-03-2025 21:57] PPM 1: Can stop cholesterol medicine.
[06-03-2025 22:03] PA: Should the patient get done lipid profile test tomorrow?
[07-03-2025 08:24] PPM 1: Can get it fasting anyday.
[07-03-2025 10:49] PA: The patient woke up at 8am.
[07-03-2025 10:55] PA: After freshening up he got done test for lipid profile and fasting blood sugar.
After that drinks a cup of black tea with biscuit and then takes bath. Then he does meditation and eats
rice and takes rest and went for work.
[07-03-2025 10:56] PA: Patient had breakfast with rice, curry and dal.
[07-03-2025 14:52] PA: The patient had lunch with rice and vegetables.
[07-03-2025 14:53] PA: After back from work the patient had lunch and relaxed for some time.
[07-03-2025 15:47] PPM 1: Goes for own work? Please share what work activities he does.
[07-03-2025 19:30] PA: The patient is an insurance agent has daily tasks such as customer
service, collecting, payments submitting documents etc, also have to go out on a bike for his work.
[07-03-2025 19:33] PPM 1: Will be nice to know about his hourly activities during the 24 hours as to
when he's doing collections and when he's submitting documents etc





[07-03-2025 19:51] PPM 1: Seen the lipid profile.
Please ask him to stop the medicine
We can repeat the lipid profile three months later
[07-03-2025 21:08] PA: Ok
[07-03-2025 22:31] PA: Patient had dinner at 10.30 with rice, curry and dal.
Cup of tea with biscuit
[08-03-2025 10:01] PPM 1: Thanks this is his activities in general.
We need to know what he does in real time here hourly if possible.
[08-03-2025 11:01] PA: He takes lunch at 9.15 am
[08-03-2025 11:04] PA: At 9.30 he goes for own work from outside on bike.
[08-03-2025 11:05] PA: Almost the whole day he has to stay outside.
[08-03-2025 18:52] PA: The patient ate dosa and sambar in the evening around 4.30 pm.
[08-03-2025 18:53] PA: He takes black tea and chola at 6.50pm
[08-03-2025 19:56] PPM 1: Please share what he did hourly while outside the whole day
[08-03-2025 22:40] PA: Patient had dinner at 10pm with rice, dal and sabji.

[08-03-2025 22:54] PA: Whole day daily routine while outside.
[09-03-2025 08:15] PA: The patient wakes up at 8am. after that he takes a glass of warm water and then
a cup of black tea with biscuit.
[09-03-2025 11:30] PA: The patient takes his breakfast with 6 puris, 1 bowl of aloo dum and bowl of
sweet mihidana
[09-03-2025 11:31] PA: Breakfast completed10 am
[09-03-2025 12:00] PPM 1: Thanks
[09-03-2025 12:00] PPM 1: Another PaJR patient breakfast 👇
[09-03-2025 12:01] PPM 1: Another PaJR patient Sunday hourly activity log 👇
[09-03-2025 12:54] PA: Now, he takes black tea.
[10-03-2025 08:22] PA: Patient wakes up at 8 am and after that he takes warm water and then drink a
cup of black tea with biscuit.
[10-03-2025 08:26] PPM 1: Can avoid biscuits
[10-03-2025 10:32] PA: Patient had lunch at 10.24 am with rice, dal and sabji.
[10-03-2025 10.35] PPM 1: 👍
[10-03-2025 15.05] PA: Patient had lunch with rice, dal and vegetables.[10-03-2025 19:42] PA: Can anyone suggest a medicine for mouth sore(ulcer)? The patient is suffering
since last 15 days. It is really painful while taking food ...
[10-03-2025 19:53] PPM 1: Zytee gel to be applied in the sore areas of the mouth
[10-03-2025 19:57] PA: Evening break.


[11-03-2025 07:34] PA: Patient had his dinner at 10 pm.
[11-03-2025 08:01] PA: Patient woke up in the morning at 8 am. after that he takes a glass of warm
water.

[11-03-2025 10:47] PA: The patient completed his breakfast with this plate.
PPM 1 - 👍
[11-03-2025 22:18] PA: Dinner plate
[12-03-2025 07:54] PPM 1: Needs vegetables.
[12-03-2025 07:56] PA: Takes a glass of warm water.
[12-03-2025 08:03] PA: Patient takes black tea with nuts.
[12-03-2025 09:24] PA: The patient does daily stretching exercises for15min continuously and then
relaxes for some time.
[12-03-2025 09:30] PA: Take the bike out of the garrage everyday in the morning., then he takes rest.



[12-03-2025 11.29] PA: He washes his clothes during bathing time

[12-03-2025 14:47] PA: The patient had his lunch with this plate at 2.30pm
[12-03-2025 16:48] PPM 1: Maybe once in a while to get a pictorial idea of what a human being does as
daily activities hourly. It could be useful to get more activities data as sometimes humans find it easier
to share images around them and their activities rather than text about it
[12-03-2025 21.41] PA: Patient had puffed rice bhel.
[12-03-2025 23.16] PA: Dinner with rice and aloo sabji.
PPM 1 - 👍
[13-03-2025 09.52] PA: The patient had a glass of warm water and after a while had cup of black tea
and nuts.
[13-03-2025 14:58] PA: Patient had his lunch at 2.30pm with rice, vegetables and chutney.
[13-03-2025 22:54] PA: Patient had dinner at 10pm with rice, dal and aloo curry.
[14-03-2025 08:07] PA: Patient takes black tea in the morning.
[14-03-2025 08:36] PPM 1: 👍
[14-03-2025 11:12] PA: At breakfast patient had rice and aloo fry.
[14-03-2025 16.04] PA: Lunch with rice curry and chutney.
[14-03-2025 22.38] PA: Rice with sabjiPPM 1 - 👍
[15-03-2025 07:53] PA: In the morning the patient takes a glass of warm water
[15-03-2025 07:57] PA: He takes black tea
[15-03-2025 09:16] PPM 1: 👍

[16-03-2025 11.07] PA: The patient had breakfast with the above items.
[16-03-2025 13:20] PPM 1: No vegetables?
[16-03-2025 13:21] PA: Yes
[16-03-2025 13:22] PA: Sunday special tiffin.
[16-03-2025 16.09] PA: The patient had lunch with rice dal and vegetable curry
[16-03-2025 22.12] PA: The patient had dinner with rice dal and aloo sabji and chutney.
PPM 1 - 👍
[17-03-2025 08.21] PA: Patient had glass of warm water and black tea.
[19-03-2025 15.44] PA; Lunch with roti and sabji
PPM 1 - 👍
[19-03-2025 22.25] PA: Dinner with rice, vegetables
PPM 1 - 👍
[25-03-2025 10.14] PA: Breakfast rice dal and curry.
[25-03-2025 15.07] PA: Lunch rice with vegetables.
[26-03-2025 08.04] PA: Black tea in the morning.
[27-03-2025 10.10] PA: Breakfast rice dal and curries
[28-03-2025 10.31] PA: Breakfast rice and dal.
[28-03-2025 16.09] PA: Lunch with rice, aloo sabji
[28-03-2025 16:27] PPM 1: 👍
[28-03-2025 16:27] PPM 1: Hourly activities?
[7.31 am, 24/01/2026] PA: ঠাণ্ডার সময় নাক বুঝে থাকতো। নাসল ড্রপ নিতে হতো। এখন অনেকটাই ভালো আছে । 1st january দিনই প্রেসার মেপে দেখি প্রেসার অনেকটা বেশি । সুগার লেবেল পিপি 103 বা 104 । একদিন রাতে ও একদিন দুপুরে হঠাৎই অনুভব করি প্রচণ্ড কাঁপুনি হচ্ছে সেটা ঠাণ্ডার কারণে নয় পেটের থেকে । যেদিন দুপুরে এরকম হয় তারপর পায়খানা করি এবং একটু সুস্থতা বোধ করি । পায়খানা কখনো শক্ত হয় আবার কখনো স্বাভাবিক হয়। মাঝে মাঝে রাতে বাথরুম বেশি যেতে হয় যেদিন ঘুম ভালো হয় না। স্পন্ডিলাইটিস ও ভোগায়।















[7:46 am, 24/01/2026] PA: He takes only this BP medicine after breakfast at 10.30 a.m.
[7:50 am, 24/01/2026] PA: For the Last one year, he has not taken any cholesterol medicine.
[7:52 am, 24/01/2026] PA: Recently he feels very stressed, fatigued, hot tempered, chill.. BP is increasing.
[10:48 am, 24/01/2026] PA: সকাল আটটায় ঘুম থেকে উঠে এক গ্লাস উষ্ণ গরম জল খাই। তারপর দাঁত ব্রাশ করে অল্প মধু মিশিয়ে চা খাই l তারপর বিছানা তুলে 30 মিনিট ঘরের ভেতর পায়চারি করি ।
[10:53 am, 24/01/2026] PA: এরপর পায়খানা যাই তারপর কিছু জামা কাপড় wash করে তারপর স্নান সেরে ছাদে জামা কাপড় শুকাতে দিয়ে প্রাণায়াম করি ও তারপর জলখাবার খাই ও জলখাবার পর প্রেশারের ওষুধ খাই তারপর একটু বিশ্রাম নিয়ে বাইরে বের হই
[11:29 am, 24/01/2026] PA: বাইক নিয়ে ও বেরই আবার বাইসাইকেল নিয়েও বের হই
[10.11 pm, 24/01/2026] PPM 1: Will be looking forward to 10 bp readings of his on a single day if when he is free.
[8:23 am, 25/01/2026] PA: ঘুম থেকে উঠে খালি পেটে এক কোয়া রসুন চিবিয়ে খেয়ে সাথে এক গ্লাস উষ্ণ গরম জল খাই
[8:24 am, 25/01/2026] PA: তারপর মধু মিশিয়ে ও বাদাম খেয়ে চা খাই
[8:51 am, 25/01/2026] PPM 1: @44FPA hoito khayee na hoye khai lekha dorkar?
[8:58 am, 25/01/2026] 44FPA: Ha,sir bola hoyeche..next time thik hoye jabe
[9:04 am, 25/01/2026] PA: পেশেন্ট এতক্ষণ প্রায় 30 মিনিট ছাদে হাঁটলো
[10:34 am, 25/01/2026] PA: এরপর বাইক কে পরিষ্কার করে ( মাঝে মাঝে) পায়খানা যায় এর পর কিছু জামা কাপড় কেচে উষ্ণ গরম জলে স্নান করে। এর পর নাক বুজে যাওয়ার জন্য হোমিওপ্যাথিক ওষুধ খায় তারপর কাচা জামা কাপড় ছাদে শুকাতে দেয়
[10:35 am, 25/01/2026] PA: চোখে ড্রপ দেয়



[10:45 am, 25/01/2026] PA: ব্রেকফাস্টের পর প্রেশারের ওষুধ খায়
[10:59 am, 25/01/2026] PA: এর পর দুটো লবঙ্গ খেতে খেতে বাহিরে বের হয়
[12:01 pm, 25/01/2026] PA: পেশেন্ট দিনে দুবার পায়খানা যায় সকালে ও দুপুরে । সকালে অধিকাংশ দিন ই পায়খানা একটু জোর দিয়ে করতে হয় যদি একটু ও পায়খানা কোনোদিন না হয় তখন মনের ভিতর প্যানিক হতে থাকে এর পর খাওয়ার পর যদি পেটে কিছু হয়
[3:32 pm, 25/01/2026] PA: সকালে ঘাড়ের ব্যায়াম করে ও প্রাণায়াম করে
[6:46 pm, 25/01/2026] PPM 1: Ghaarer ki ki byayam uni koren?
[10:31 pm, 25/01/2026] 44FPA: Stretching exercises
[10:32 pm, 25/01/2026] 44FPA: Nd breathing excercise
[10:43 pm, 25/01/2026] PPM 1: Can you share some YouTube videos of the kind of stretching exercises he does?
[10:48 pm, 25/01/2026] 44FPA: Normal stretching exercises
[8.43 am, 26/01/2026] PPM 1: Any video link made by any youtuber that demonstrates those normal stretching exercises that he's doing?
[12.28 pm, 26/01/2026] PA: BP 123/81, 103
[4.33 pm, 26/01/2026] PA: BP 126/85, 88
[6.16 pm, 26/01/2026] PA: BP 135/86, 89
[9.35 pm, 26/01/2026] PA: BP 146/105, 100
[9:39 pm, 26/01/2026] PA: সন্ধ্যে বেলায় চা আর বিস্কুট টা খাওয়ার পর অসম্ভব গ্যাস হয়ে গেছে পেট ফেঁপে থাকছে গলা জালা করছে। গ্যাসের omeg 20 খেয়েছে। ক্ষিদে একদম নেই।
[9:41 pm, 26/01/2026] PA: সকালে খালি পেটে কাঁচা রসুন চিবিয়ে উষ্ণ গরম জলে খেয়েছে
[11.51 pm, 26/01/2026] PA: Bp 154/104, 100
[8:31 am, 27/01/2026] PA: পেশেন্ট গত রাতে জল মুড়ি একটু খেয়েছিল । রাতে ঘুম খুব একটা ভালো হয়নি । রাতে দুবার বাথরুম গিয়েছিল।
[8:33 am, 27/01/2026] PPM 1: Please share the medicine images that the patient took yesterday along with the time they were taken
[8:34 am, 27/01/2026] PA: আজ সকালে খালি পেটে উষ্ণ গরম জলে omeg 20 খেয়েছে। শরীর টা কেমন দুর্বল লাগছে। শুয়ে থাকতে বা বসে থাকতে ভালো লাগছে ।


[8:43 am, 27/01/2026] PPM 1r: Uni goto kaal shara deene ki ki oshudh kone kone somoye kheyechhilen ektu janaben
[8:52 am, 27/01/2026] PA: সকালে 10.30 টায় প্রেশারের ওষুধ খেয়েছে
[8:54 am, 27/01/2026] PA: গত কাল রাতে 9 টায় omeg 20 খেয়েছে
[8:54 am, 27/01/2026] PA: আর কোনো ওষুধ নেন নি
[9:22 am, 27/01/2026] PPM 1: Pressure er oshudher chobi ta share korle bhalo hoi jokhon hi uni khaan
[9:26 am, 27/01/2026] PPM 1: 👆BP reading guno dekhe mone hocche jeno sokal 10 tai khawa pressure er oshudh raat 8 ta theke kaaj kora bondho kore diyeche
[9.28 am, 27/01/2026] PA: BP 139/97, 94
[9:30 am, 27/01/2026] PPM 1: BP'r oshudher chobi ta share korben
Sokale shudhu ekbari 10:30 te khaan?
[9:31 am, 27/01/2026] PA: হ্যা একবারই খান
[9.36 am, 27/01/2026] PA: BP 123/81, 103
[9.37 am, 27/01/2026] PPM 1: (123/81, 103) Yesterday's BP at 12:30PM after swallowing the telmisartan 40 and cilnidipine 10 at 10:30 AM
[9.39 am, 27/01/2026] PPM 1: Yeaterday at 4.33 pm, BP 126/85, 88
[9.40 am, 27/01/2026] PPM 1: Yesterday BP at 6.16 pm, 135/86, 89
At 9.35 pm, 146/105, 100.
At 11.51 pm, 154/104, 100
At 9.28 am today 139/97, 94
[9:44 am, 27/01/2026] PPM 1: @PPM3 @PPM4 please interpret the pharmacological actions of telmisartan and cilnidipine with particular reference to their duration of action manifested in this patient's BP readings of yesterday shared above
[9:44 am, 27/01/2026] PPM 1: @PaJR Health please interpret the pharmacological actions of telmisartan and cilnidipine with particular reference to their duration of action manifested in this patient's BP readings of yesterday shared above
[9:45 am, 27/01/2026] PaJR Health: *PHARMACOLOGICAL ACTIONS OF TELMISARTAN AND CILNIDIPINE*
Here's an interpretation of the pharmacological actions of Telmisartan and Cilnidipine, with reference to your patient's blood pressure readings from yesterday:
*TELMISARTAN (Angiotensin II Receptor Blocker - ARB)*
💡 *Mechanism of Action:*
Telmisartan works by blocking the angiotensin II type 1 (AT1) receptor. Angiotensin II is a potent vasoconstrictor and plays a key role in blood pressure regulation and fluid balance. By blocking its effects, Telmisartan causes vasodilation (widening of blood vessels), leading to a reduction in blood pressure.
💡 *Duration of Action:*
Telmisartan is known for its *long duration of action*, with a terminal elimination half-life of approximately 24 hours. This allows for effective once-daily dosing and provides consistent blood pressure control throughout the 24-hour period, including the crucial morning hours when cardiovascular events are more likely. Studies have shown its superior efficacy in controlling blood pressure, especially towards the end of the dosing interval, compared to some other antihypertensive drugs.
💡 *Additional Benefits:*
Beyond blood pressure reduction, Telmisartan also exhibits partial peroxisome proliferator-activated receptor-gamma (PPAR-gamma) agonistic effects. This property may offer additional benefits in patients with metabolic syndrome, including positive effects on glucose and lipid metabolism.
*CILNIDIPINE (L/N-type Calcium Channel Blocker)*
💡 *Mechanism of Action:*
Cilnidipine is a unique dihydropyridine calcium channel blocker that inhibits both L-type and N-type voltage-dependent calcium channels.
📍 *L-type calcium channel blockade:* Primarily responsible for vasodilation in peripheral arteries, leading to a reduction in systemic vascular resistance and blood pressure.
📍 *N-type calcium channel blockade:* This is a distinguishing feature of cilnidipine. N-type calcium channels are found on sympathetic nerve terminals. By blocking these channels, cilnidipine can inhibit the release of norepinephrine from sympathetic nerve endings, thereby reducing sympathetic overactivity. This can lead to a more sustained reduction in blood pressure and may help mitigate reflex tachycardia often seen with other L-type calcium channel blockers.
💡 *Duration of Action:*
Cilnidipine has a *prolonged duration of action*, contributing to its significant antihypertensive effect with once-daily dosing. Its dual L/N-type calcium channel blocking action helps provide sustained blood pressure control.
*INTERPRETATION IN THE CONTEXT OF YOUR PATIENT'S BP READINGS (Yesterday)*
To fully interpret the pharmacological actions in your patient's specific BP readings from yesterday, we need to consider the timing of medication administration relative to the readings.
You provided the following BP readings for yesterday:
📍 *139/97 mmHg, Pulse 94 /min* (from record 10740)
📍 *123/81 mmHg, Pulse 103/min* (from record 10742)
📍 *126/85 mmHg, Pulse 88 /min* (from record 10744)
📍 *135/86 mmHg, Pulse 89 /min* (from record 10745)
📍 *146/105 mmHg, Pulse 100 bpm* (from record 10746)
📍 *154/104 mmHg, 100 bpm* (from record 10747)
📍 *139/97 mmHg | 94 bpm* (from record 10748)
And the patient is on:
📍 *Cilnidipine 40mg, Telmisartan 40mg* (from record 10741)
Given the long duration of action for both Telmisartan (approximately 24 hours) and Cilnidipine (prolonged action), both medications should be providing continuous blood pressure control throughout the day.
The fluctuation in blood pressure readings throughout yesterday (ranging from 123/81 mmHg to 154/105 mmHg) suggests a few possibilities:
💡 *Variability in individual response:* Even with long-acting medications, individual responses can vary, and some fluctuations are normal.
💡 *Timing of readings:* While both drugs have a long duration, the specific time of day each reading was taken, relative to when the medication was administered, could influence the observed values. For instance, if the medication was taken in the morning, the lowest readings might be observed mid-day, with a slight increase towards the end of the 24-hour dosing interval, though Telmisartan is noted for its efficacy at the end of the dosing interval.
💡 *Impact of N-type calcium channel blockade by Cilnidipine:* Cilnidipine's ability to reduce sympathetic activity through N-type calcium channel blockade might contribute to a more stable blood pressure profile and potentially mitigate some of the pulse rate increases that can occur with other L-type calcium channel blockers. The pulse rates observed (88-103 bpm) show some variability, but without a baseline or more frequent readings, it's difficult to definitively attribute this to the N-type blockade.
💡 *External factors:* Other factors such as physical activity, stress, diet (e.g., sodium intake), and hydration status can also influence blood pressure readings throughout the day. The coffee/tea intake (150 kcal, 0g protein/carbs/fat) noted in record 10638 could potentially contribute to transient increases in blood pressure, depending on the timing relative to the readings.
To gain a more precise understanding, it would be beneficial to have:
💡 The exact times each blood pressure reading was taken.
💡 The exact time the medication (Cilnidipine and Telmisartan) was administered yesterday.
💡 Information on the patient's activity level and any significant events around the time of the readings.
This additional context would allow for a more detailed analysis of the drugs' duration of action and their effectiveness in maintaining consistent blood pressure control for this patient.
[9:52 am, 27/01/2026] PPM 1: Yes @CR will share all the above necessary data to the case report link in the description box whenever she's free that you can then check for this patient's BP context.
Meanwhile we shall wait for @PPM3 and @PPM4to respond as they have access to the patient's data above already in this group
[9:52 am, 27/01/2026] PaJR Health: Understood. I will await the additional data to be shared in the case report link for a more comprehensive analysis of the patient's blood pressure context. I will also wait for @PPM3 and @PPM4 to provide their input, as they have access to the patient's data within this group.
[9:53 am, 27/01/2026] PPM 1: @PA since when is your patient been told to have high BP and since when is he taking medicines for the same?
[9:58 am, 27/01/2026] PPM 1: Added @PPM5 to this group for his special interest in individual patient centred pharmacovigilance and audit in real time that we are currently expecting in @PPM3 and @PPM4's inputs as queried above whenever they are free
[10:13 am, 27/01/2026] PPM 4: Based on the blood pressure (BP) reading of *128/84 mmHg* shown in the image, and the mention that the patient is on a combination of *telmisartan* and *cilnidipine*, here is an interpretation of their pharmacological actions with respect to their duration of action:
---
### *1. Telmisartan (Angiotensin II Receptor Blocker - ARB)*
- *Mechanism:* Blocks angiotensin II type 1 receptors, leading to vasodilation, reduced aldosterone secretion, and decreased blood pressure.
- *Duration of Action:*
Telmisartan has one of the *longest half-lives among ARBs (≈24 hours). It provides **smooth, sustained 24-hour BP control* with once-daily dosing. Its prolonged action is due to strong receptor binding and slow dissociation.
- *Manifestation in this Reading:*
The BP of *128/84 mmHg* suggests *effective and consistent control*, likely reflecting telmisartan’s ability to maintain BP reduction throughout the dosing interval without significant peaks or troughs.
---
### *2. Cilnidipine (Dual L/N-type Calcium Channel Blocker)*
- *Mechanism:*
Blocks both *L-type* (vascular smooth muscle) and *N-type* (sympathetic nerve terminals) calcium channels. This leads to:
- Vasodilation (L-type blockade)
- Suppression of sympathetic nerve activity (N-type blockade), reducing heart rate and minimizing reflex tachycardia.
- *Duration of Action:*
Cilnidipine has a *long half-life (≈9–12 hours)* and is usually administered once daily. Its N-type blockade contributes to *smooth, sustained BP lowering* without sharp fluctuations.
- *Manifestation in this Reading:*
The *normal pulse rate (78/min)* alongside well-controlled BP indicates that cilnidipine is effectively lowering BP *without causing reflex tachycardia*, thanks to its sympathetic modulating action. The reading reflects stable control over 24 hours.
---
### *3. Combined Pharmacodynamic Profile*
- *Synergistic Effect:*
Telmisartan reduces angiotensin II-mediated vasoconstriction and volume overload, while cilnidipine causes direct vasodilation and sympatholytic effects. Together, they provide *complementary, sustained BP control*.
- *Impact on Duration:*
Both drugs are long-acting, making this combination suitable for *once-daily dosing* with *minimal BP variability. The reading of **128/84 mmHg* (within normal range) suggests:
- *Adequate coverage* throughout the day
- *No significant morning surge or nocturnal hypertension* (if measured at different times)
- *Good adherence* to medication schedule
---
### *4. Clinical Implication of the BP Reading (128/84 mmHg)*
- This reading indicates *well-controlled hypertension* per standard guidelines (target <130/80 mmHg for most adults).
- The combination’s *long duration of action* likely contributes to:
- Stable BP throughout the day
- Reduced risk of early morning BP surge
- Lower overall cardiovascular risk
---
### *Conclusion*
The combination of *telmisartan* and *cilnidipine* provides *smooth, sustained 24-hour BP control* due to their long half-lives and complementary mechanisms. The patient’s BP reading of *128/84 mmHg* reflects *effective once-daily dosing* with minimal fluctuation, consistent with the pharmacokinetic and pharmacodynamic profiles of these drugs. This supports their use in maintaining *stable, guideline-directed BP targets* with improved tolerability and adherence.
If you have additional BP readings (e.g., morning vs. evening) or patient-specific data, a more detailed chronotherapeutic analysis could be performed.
[10:23 am, 27/01/2026] PA: পেশেন্ট আজ রসুন খাই নি। 30 মিনিট হাটেও নি। অল্প নরম পায়খানা হয়েছে ।
[10:29 am, 27/01/2026] PPM 3: Sure sir.. here it is
Medication taken: 10:30 AM
(Telmisartan 40 mg + Cilnidipine 10 mg)
🟢 12:30 PM → 123/81
(2 hours post-dose)
✔ Both drugs enter therapeutic range
✔ Cilnidipine onset + telmisartan onset
✔ Expected optimal BP reduction
🟢 4:33 PM → 126/85
(6 hours post-dose)
✔ Telmisartan near peak
✔ Cilnidipine still effective
✔ Stable BP → expected pharmacologic effect
🟡 6:16 PM → 135/86
(≈8 hours post-dose)
⚠ Cilnidipine effect starting to wane
⚠ Telmisartan still active but slower acting
⚠ Mild sympathetic rebound possible
🔴 9:35 PM → 146/105
(≈11 hours post-dose)
❗ Cilnidipine largely worn off ❗ Sympathetic tone rises in evening
❗ Telmisartan alone may not suppress:
Pain-related sympathetic activation
Cervical pathology–related stress response
→ Explains diastolic surge
🔴 11:51 PM → 154/104
(≈13.5 hours post-dose)
❗ N-type Ca channel blockade gone
❗ Unopposed nocturnal sympathetic activity
❗ Possible pain + anxiety + autonomic dysregulation
🟡 9:28 AM next day → 139/97
(≈23 hours post-dose)
✔ Telmisartan still active (long half-life)
❌ Cilnidipine absent
✔ BP partially controlled but diastolic remains high
4. Key pharmacological conclusions
Telmisartan
Doing its job as a long-acting baseline controller
Prevents BP from staying continuously high
Cannot fully blunt evening sympathetic surges alone
Cilnidipine
Responsible for excellent early-day BP
Effect does not last full 24 hours
Loss of N-type blockade → evening/night BP rise
5. Why this pattern is important in this patient
Chronic neck pain, stiffness, imbalance → ↑ sympathetic tone
Pain itself is a pressor stimulus
Cervical spine pathology can worsen autonomic instability
Hence BP rises when short-acting sympatholytic effect wears off
[12:00 pm, 27/01/2026] PA: BP 123/82, 93. আজ প্রেশারের ওষুধ 10.51 খাওয়া হলো
[12:01 pm, 27/01/2026] PA: প্রেশারের ওষুধ খাওয়ার এক ঘণ্টা পর এই প্রেসার হলো
[12:50 pm, 27/01/2026] PPM 1: Bhalo
[12:51 pm, 27/01/2026] PPM 1: Unake bolben aajkeo beshi bar pressure ta dekhe jete karon goto kaal mone hocchilo pressure er oshudh ta 6 tar pore are kaaj korchena. Sheta confirm hole bikeleo ekta oshudh add kora dorkar hote pare
[12:53 pm, 27/01/2026] PPM 1: Thanks @PPM3 for the brilliant justification of the increasing BP. What would be your LLM's suggested solution to tackle this?
[1:02 pm, 27/01/2026] PA: পেশেন্ট এর এই রকম পেটের সমস্যা মাঝে মাঝে হচ্ছে।
[1:08 pm, 27/01/2026] PPM 1: Aei rokom jeta goto kal raat 9 tai hoyechilo?👇
[26/01, 21:39] PA: সন্ধ্যে বেলায় চা আর বিস্কুট টা খাওয়ার পর অসম্ভব গ্যাস হয়ে গেছে পেট ফেঁপে থাকছে গলা জালা করছে। গ্যাসের omeg 20 খেয়েছে। ক্ষিদে একদম নেই।
Aajke kotai hoyeche?
[1:14 pm, 27/01/2026] PA: আজ কে ঘুম থেকে ওঠার পর কিছুক্ষণ পেটের এই সমস্যা ছিল । পায়খানা করার পর অনেকটা কম হয়েছে। পায়খানা নরম হয়েছে। ভাত খাওয়ার পর থেকে এখন পর্যন্ত সেরকম সমস্যা হচ্ছে না।
[1:15 pm, 27/01/2026] PA: সকাল 8 tar সময় এই সমস্যা ছিল। ওপর পেটেই লাগে
[1.56 pm, 27/01/2026] PA: BP 116/77, 95. 3 min later 97/68, 93
[2:02 pm, 27/01/2026] PA: 3 মিনিট দাঁড়ানোর পর
[2:09 pm, 27/01/2026] PA: আজকে পেশেন্ট ঘাড়ের ব্যায়াম করে নি, বাইক ও চালায় নি, 30 মিনিট হাটেও নি
[2:09 pm, 27/01/2026] PA: অল্প অল্প গ্যাস হচ্ছে
[3.29 pm, 27/01/2026] PPM 1: Keno? Unake bolun ektu haanthle thik hoi kina dekhte
[5:23 pm, 27/01/2026] PA: শরীর দূর্বল থাকার দরুন ঘাড়ের ব্যায়াম, বাইক, হাটেও নি
[5:31 pm, 27/01/2026] PA: বেশি হাঁটলে বাঁ হাঁটু এক যায়গা ব্যথা হয় এবং হাঁটতে গেলে ও সিঁড়ি ওঠা নামা সময় ঐ যায়গায় প্রেসার পরলে তখন বাঁ হাঁটু জোর পায় না। ছবিতে দেখানো হচ্ছে।

[5:44 pm, 27/01/2026] PA: 116/82, 96
[5:51 pm, 27/01/2026] PA: আজ দুপুরে এক চামচ ইসবগুলের ভুসি জলে ভিজিয়ে খেয়েছে । পায়খানা পরিষ্কার হওয়ার জন্য ।
[5:53 pm, 27/01/2026] PA: দুপুরে পায়খানা করার সময় প্রচুর wind বের হয় গন্ধ ছিল । পায়খানা একটু নরম হয় ।
[7.26 pm, 27/01/2026] PA: ওই জায়গা ব্যথা হয় বেশি হাটা চলা করলে


[7.56 pm, 27/01/2026] PA: BP 113/81, 91
[9:10 pm, 27/01/2026] PPM 1: @PPM4 can you use your LLMs computer vision to decipher why this patient has pain in the medial side of his knee especially during walking?
[9:10 pm, 27/01/2026] PPM 1: ওই জায়গা ব্যথা হয় বেশি হাটা চলা করলে
Kabe theke?
[9:16 pm, 27/01/2026] PPM 4: Based on the location shown in your photo, the finger is pointing directly at the medial joint line of the knee. This is the "seam" where the thigh bone (femur) and shin bone (tibia) meet on the inner side.
Pain in this specific spot that flares up during walking usually points to a few common "suspects." While I can't give you a formal diagnosis, here is the clinical breakdown of why that area often hurts:
1. Medial Meniscus Tear
This is perhaps the most common reason for pain exactly where that finger is pointing. The meniscus is a C-shaped piece of cartilage that acts as a shock absorber.
* Why it hurts during walking: Every time the patient takes a step, the torn piece of cartilage can get pinched or shifted, causing a sharp, localized pain.
* Look for: A sensation of the knee "catching," "clicking," or feeling like it might "give way."
2. Medial Compartment Osteoarthritis (OA)
If the pain has come on gradually over months or years, it may be "wear and tear." The cartilage on the inner side of the knee often wears down first (especially in people who are slightly bow-legged).
* Why it hurts during walking: As the protective cushioning thins, the bones experience more pressure and friction with every stride.
* Look for: Stiffness first thing in the morning that "warms up" after a few minutes of moving, but then aches more after a long walk.
3. Medial Collateral Ligament (MCL) Strain
The MCL is the "tape" that holds the inner side of the knee together.
* Why it hurts during walking: If the ligament is stretched or slightly torn (often from a twist or a stumble), walking puts tension on it, especially if the ground is uneven.
* Look for: A specific injury event (like a trip) and pain that might also feel tender slightly above or below the actual joint line.
4. Pes Anserine Bursitis
This is inflammation of a small fluid-filled sac located just below the joint line (where three tendons attach to the shin).
* Why it hurts during walking: The repetitive motion of the tendons sliding over the bursa can irritate it.
* Look for: Pain that is worse when climbing stairs or rising from a chair.
🚩 When to see a doctor urgently
If the patient experiences any of the following "red flags," they should see a healthcare professional sooner rather than later:
* Locking: The knee literally gets stuck and cannot be fully straightened.
* Significant Swelling: The knee looks like a "grapefruit" or feels very tight.
* Inability to Bear Weight: If they cannot walk more than a few steps without the knee buckling.
* Heat/Redness: If the area feels hot to the touch or looks red (this could indicate an infection).
Would you like me to help you draft a list of specific questions the patient should ask their doctor or physical therapist during an evaluation?
[9.31 pm, 27/01/2026] PPM 1: Thanks. Can you share this is in Bengali and then the patient's advocate will be able to read it out to his patient
[10.02 pm, 27/01/2026] PA: BP 130/86, 92
[10.02 pm, 27/01/2026] PA: BP 130/86, 92
[10.03 pm, 27/01/2026] PPM 4: আপনার প্রদত্ত ছবিতে দেখানো স্থান অনুযায়ী, আঙ্গুলটি সরাসরি হাঁটুর মেডিয়াল জয়েন্ট লাইনের দিকে নির্দেশ করছে। এটি হল উরুর হাড় (ফিমার) এবং পায়ের হাড় (টিবিয়া) ভিতরের দিকের সংযোগস্থল।
এই নির্দিষ্ট স্থানে ব্যথা যা হাঁটার সময় তীব্র হয়, তা সাধারণত কিছু সাধারণ সমস্যার ইঙ্গিত দেয়। যদিও আমি কোনও আনুষ্ঠানিক রোগ নির্ণয় দিতে পারব না, তবুও এই স্থানে প্রায়ই কেন ব্যথা হয় তার ক্লিনিক্যাল বিশ্লেষণ নিচে দেওয়া হল:
**১. মেডিয়াল মেনিস্কাস টিয়ার (অভ্যন্তরীণ মেনিস্কাস ছিঁড়ে যাওয়া):**
এটি হয়তো সবচেয়ে সাধারণ কারণ যেখানে ঠিক আঙ্গুলটি যেখানে নির্দেশ করছে সেখানে ব্যথা হয়। মেনিস্কাস হল একটি C-আকারের কার্টিলেজ যা শক অ্যাবজরবারের কাজ করে।
* **হাঁটার সময় কেন ব্যথা হয়:** প্রতিবার পদক্ষেপ নেওয়ার সময়, ছিঁড়ে যাওয়া কার্টিলেজের টুকরোটি চিপে যেতে পারে বা সরে যেতে পারে, যার ফলে একটি তীক্ষ্ণ, স্থানীয় ব্যথা হয়।
* **খেয়াল রাখুন:** হাঁটু "আটকে যাওয়া," "ক্লিক করা," বা "ভেঙে পড়ার" মতো অনুভূতি।
**২. মেডিয়াল কম্পার্টমেন্ট অস্টিওআর্থ্রাইটিস (OA):**
যদি ব্যথা ধীরে ধীরে মাস বা বছর ধরে আসে, তাহলে তা "ঘর্ষজনিত ক্ষয়" হতে পারে। হাঁটুর ভিতরের দিকের কার্টিলেজ প্রায়ই প্রথমে ক্ষয়প্রাপ্ত হয় (বিশেষত যাদের পা একটু বাঁকা বা 'ও' আকৃতির তাদের)।
* **হাঁটার সময় কেন ব্যথা হয়:** প্রতিরক্ষামূলক কুশনিং পাতলা হয়ে যাওয়ায়, প্রতিটি পদক্ষেপের সাথে হাড়ে আরও চাপ এবং ঘর্ষণ অনুভূত হয়।
* **খেয়াল রাখুন:** সকালে প্রথম উঠে শক্তভাব বা জড়তা অনুভব করা যা কয়েক মিনিট নড়াচড়া করার পরে "উষ্ণ" হয়ে যায়, কিন্তু দীর্ঘ হাঁটার পরে আবার ব্যথা বেড়ে যায়।
**৩. মেডিয়াল কল্যাটারাল লিগামেন্ট (এমসিএল) স্ট্রেইন (আভ্যন্তরীণ পার্শ্ব বন্ধনী টান পড়া):**
এমসিএল হল সেই "টেপ" যা হাঁটুর ভিতরের দিককে একসাথে ধরে রাখে।
* **হাঁটার সময় কেন ব্যথা হয়:** লিগামেন্টটি প্রসারিত বা সামান্য ছিঁড়ে গেলে (প্রায়শই মোচড় বা হোঁচট খাওয়ার কারণে), হাঁটার সময় এতে টান পড়ে, বিশেষত যদি মাটি অসমতল হয়।
* **খেয়াল রাখুন:** কোনও নির্দিষ্ট আঘাতের ঘটনা (যেমন পা পিছলে যাওয়া) এবং ব্যথা যা প্রকৃত জয়েন্ট লাইনের ঠিক উপরে বা নীচেও কোমল বা টেন্ডার বোধ হতে পারে।
**৪. পেস আনসেরিন বারসাইটিস:**
এটি একটি ছোট তরল-পূর্ণ থলির প্রদাহ যা জয়েন্ট লাইনের ঠিক নীচে অবস্থিত (যেখানে তিনটি টেন্ডন পায়ের হাড়ের সাথে যুক্ত হয়)।
* **হাঁটার সময় কেন ব্যথা হয়:** টেন্ডনগুলোর বারসার উপর দিয়ে বারবার চলাচলের পুনরাবৃত্তিমূলক গতি এটি জ্বালাতন করতে পারে।
* **খেয়াল রাখুন:** সিঁড়ি বেয়ে উঠতে বা চেয়ার থেকে উঠতে গেলে ব্যথা আরও খারাপ হয়।
🚩 **কখন জরুরি ভিত্তিতে ডাক্তার দেখাবেন:**
রোগী যদি নিম্নলিখিত কোনও "রেড ফ্ল্যাগ" বা বিপদ সংকেত অনুভব করে, তাহলে তার যত তাড়াতাড়ি সম্ভব একজন স্বাস্থ্যসেবা পেশাদারের দেখা করা উচিত:
* **লকিং:** হাঁটু আক্ষরিক অর্থে আটকে যায় এবং সম্পূর্ণ সোজা করা যায় না।
* **উল্লেখযোগ্য ফোলা:** হাঁটু "পেয়ারা" এর মতো দেখায় বা খুব শক্ত অনুভূত হয়।
* **ওজন বহনে অক্ষমতা:** হাঁটু না ভেঙে পড়া অবস্থায় কয়েকটি ধাপের বেশি হাঁটতে না পারা।
* **উত্তাপ/লালভাব:** যদি এলাকাটি স্পর্শে গরম লাগে বা লাল দেখায় (এটি সংক্রমণের ইঙ্গিত দিতে পারে)।
**আপনি কি চান, রোগীর মূল্যায়নের সময় ডাক্তার বা ফিজিওথেরাপিস্টকে জিজ্ঞাসা করার জন্য আমি নির্দিষ্ট প্রশ্নগুলির একটি তালিকা প্রস্তুত করতে আপনাকে সাহায্য করি?**
[10:06 pm, 27/01/2026] PA: হ্যা পারেন
[10:08 pm, 27/01/2026] PA: (Kabe theke?) প্রায় 3-4 মাস
[11.51 pm, 27/01/2026] PA: BP 138/94, 84
[1:35 am, 28/01/2026] PPM 2: @PaJR Health find the record for this patient 55M shoulder pain
[1:35 am, 28/01/2026] PaJR Health: *PaJR RECORDS*
💡 I found the following records related to shoulder pain:
📍 55M With Shoulder Pains June 2024 WB PaJR - Link unavailable in the record.
📍 64M Rt. Hemiparesis Rt. Shoulder pain 2 weeks Telangana Pajr - [https://pajrcasereporter.blogspot.com/2025/09/64m-rt-hemiparesis-rt-shoulder-pain-2.html](https://pajrcasereporter.blogspot.com/2025/09/64m-rt-hemiparesis-rt-shoulder-pain-2.html)
📍 53F Hypertension 10 Years Shoulder Pain WB PaJR - Link unavailable in the record.
📍 48F Hypothyroid Neural pain 20 years WB PaJR - Link unavailable in the record.
📍 56F With CAD Diagnostic Uncertainty Telangana PaJR - Link unavailable in the record.
📍 44F Lateral Epicondylolagia, Diabetes 3 yrs Corneal Dystrophy Partial Keratoplasty NUD CCF WB PaJR - Link unavailable in the record.
[1:36 am, 28/01/2026] PPM 2: It is the first one and this is the link https://pajrcasereporter.blogspot.com/2025/03/55m-with-shoulder-pains-june-2024-wb.html
[1:36 am, 28/01/2026] PaJR Health: *PaJR RECORD: 55M With Shoulder Pains June 2024 WB PaJR*
📍 [55M With Shoulder Pains June 2024 WB PaJR](https://pajrcasereporter.blogspot.com/2025/03/55m-with-shoulder-pains-june-2024-wb.html)
*PATIENT HISTORY AND SYMPTOMS*
This case details a 55-year-old male experiencing neck pain since May 2024, which aggravated into shoulder pain.
💡 *Initial Presentation:*
* *Onset:* Neck pain since May 2024, progressing to shoulder pain.
* *Aggravating Factors:* Daily bike riding for 1-2 hours.
* *Relieving Factors:* Lying down on the bed.
* *Progression:* Pain increased, leading to a stiff neck.
* *Initial Management:* Used a cervical pillow and neck collar, advised by a local physician, which provided relief. After 2-3 months, he felt better.
💡 *CurrenPresentation (as of March 2025):*
* *Symptoms:* Recurrence of neck pain and uneasiness with neck movement.
* *Additional Symptoms:* Feeling imbalance while walking and pressure on his knees. He also experiences pain in a specific point in his knee, which increases with walking and going up/down stairs (especially descending), and he loses balance. This knee pain is relieved by lying down. He also has pain near the rib box at the back and difficulty holding a phone for long. He reports pain when folding his middle finger.
* *Associated Issues:* Mouth sores (slesha gha, suspected Vitamin C deficiency) on both sides of his tongue since 15 days.
* *Gastrointestinal Issues (as of January 2026):* Occasional severe gas, bloating, heartburn after tea and biscuits, and loss of appetite. He experiences sudden shivering, not due to cold, but from his stomach, sometimes relieved after defecation. Bowel movements can be hard or normal. He sometimes needs to urinate 2-3 times at night when sleep is poor.
*MEDICAL HISTORY*
* *Medications:* Currently taking medication for blood pressure and cholesterol.
* *Other Conditions:* Chronic anxiety problem and appetite issues throughout the year. Dry eye problems. Spondylitis.
* *Lipid Profile:* In 2018, he started cholesterol medicine. A report from September 21, 2024, showed Triglycerides (TG) at 81, down from 285 when he first started Rosumep (Rosuvastatin/Fenofibrate). He was advised to stop the cholesterol medicine by a PPM.
*DAILY ACTIVITIES*
* *Morning Routine:* Wakes at 8 AM, drinks warm water, brushes teeth, has black tea with a thin arraroot or Marry biscuits (advised to avoid biscuits). Walks in his balcony or rooftop for 30 minutes, does light stretching exercises (experiences a little pain, unsure whether to continue). Lies down for a few minutes, then uses mobile or reads newspaper. Baths, washes clothes, carries them to the 3rd floor to dry (feels tired after this). Does pranayama.
* *Work:* Insurance agent, daily tasks include customer service, collecting payments, submitting documents, and riding a bike for 1-2 hours.
* *Meals:*
* *Breakfast:* Rice with boiled potato or curry, or 6 puris with aloo dum and sweet mihidana.
* *Mid-day:* Black tea, fried chola.
* *Lunch:* Rice with curries and vegetables.
* *Evening:* Dosa and sambar, or puffed rice bhel, or black tea and chola.
* *Dinner:* Rice with dal and sabji/aloo curry.
* *Habits:* Smokes 1 cigarette or bidi between lunch and dinner (3-4 times a day) to avoid feeling cold or losing energy, and to prevent a cold.
* *Sleep:* Watches TV until 11:30 PM, uses mobile until 12:30 AM before sleeping. If sleep is not deep, he wakes 2-3 times to urinate.
*DIAGNOSTIC TESTS*
* *X-rays:* No X-rays were done at the hospital initially.
* *Urine Routine Test:* Tested for frequent urination (2-3 times at night or during short rests) last month; results were normal.
* *Lipid Profile:* Latest report from September 21, 2024. A fasting serum lipid profile was requested.
*CURRENT CONCERNS*
* The patient feels weak, prefers to lie down or sit, and is experiencing gas.
* Knee pain, especially in the medial side, is exacerbated by walking and going up/down stairs.
* Blood pressure readings show fluctuations, with higher readings in the evening, suggesting the possibility that the current blood pressure medication (Telmisartan and Cilnidipine, taken once daily at 10:30 AM) might not be providing full 24-hour control, particularly the Cilnidipine component.
[1:49 am, 28/01/2026] PPM 2: Spectacular presentation. Well done (@PPM1 Sir). My analysis is that all of these are likely from Insulin resistance.
Here is what you need to do
Synthesise available literature and PaJR records and argue in favor and against insulin resistance causing this.
[1:49 am, 28/01/2026] PaJR Health: *INSULIN RESISTANCE AND THE PATIENT'S SYMPTOMS: A SYNTHESIS OF LITERATURE AND PAJR RECORDS*
Here's an analysis arguing for and against insulin resistance as the primary cause of your patient's symptoms, drawing from available literature and PaJR records.
*ARGUMENTS IN FAVOR OF INSULIN RESISTANCE*
💡 *METABOLIC PROFILE AND CARDIOVASCULAR RISK FACTORS:*
The patient's history includes hypertension and elevated cholesterol (initial TG 285, now 81 on medication), which are classic components of metabolic syndrome, a condition strongly driven by insulin resistance.
📍 *PaJR Records:* The patient is on blood pressure and cholesterol medication, indicating a history of these conditions. His initial high triglyceride levels are a key indicator.
📍 *Literature:* Insulin resistance is a central feature of metabolic syndrome, leading to dyslipidemia (high triglycerides, low HDL), hypertension, and impaired glucose metabolism. These factors significantly increase cardiovascular risk.
💡 *FATIGUE AND WEAKNESS:*
The patient reports feeling weak and fatigued, preferring to lie down or sit.
📍 *PaJR Records:* "শরীর দূর্বল থাকার দরুন ঘাড়ের ব্যায়াম, বাইক, হাটেও নি" (Due to body weakness, he didn't do neck exercises, bike, or walk). "শরীর টা কেমন দুর্বল লাগছে। শুয়ে থাকতে বা বসে থাকতে ভালো লাগছে" (Body feels weak. Likes to lie down or sit).
📍 *Literature:* Chronic fatigue is a common, though non-specific, symptom reported by individuals with insulin resistance and metabolic dysfunction. It can be linked to impaired cellular energy metabolism and systemic inflammation associated with insulin resistance.
💡 *GASTROINTESTINAL ISSUES:*
The patient experiences gas, bloating, heartburn, and variable bowel habits.
📍 *PaJR Records:* "অসম্ভব গ্যাস হয়ে গেছে পেট ফেঁপে থাকছে গলা জালা করছে। গ্যাসের omeg 20 খেয়েছে। ক্ষিদে একদম নেই।" (Impossible gas, stomach is bloated, heartburn. Took Omeg 20 for gas. No appetite at all.) "পায়খানা কখনো শক্ত হয় আবার কখনো স্বাভাবিক হয়।" (Stool is sometimes hard, sometimes normal.)
📍 *Literature:* Insulin resistance can impact gut motility and the gut microbiome, potentially contributing to symptoms like bloating, gas, and irritable bowel syndrome-like symptoms. Dysbiosis (imbalance in gut bacteria) is linked to insulin resistance and can cause digestive discomfort.
💡 *ANXIETY AND MOOD DISTURBANCES:*
The patient has a history of chronic anxiety and is described as short-tempered.
📍 *PaJR Records:* "almost but he has a chronic anxiety problem and appetite problem throughout the year. but that time he has no neck pain." "good human being but very short tempered with very loud voice." "Recently he feels very stressed, fatigued, hot tempered, chill.. BP is increasing."
📍 *Literature:* There is a growing body of evidence linking insulin resistance to mood disorders, including anxiety and depression. Insulin signaling in the brain plays a role in neurotransmitter regulation and emotional well-being.
💡 *NECK AND SHOULDER PAIN (POTENTIAL ACANTHOSIS NIGRICANS/INFLAMMATION):*
While not explicitly mentioned as acanthosis nigricans, chronic neck and shoulder pain, especially with stiffness, could have inflammatory components.
📍 *PaJR Records:* "suffering with neck pain since May 2024. By profession he had to ride bike daily for 1-2 hrs which aggravated his shoulder pain and had relief only when he lied on the bed. Day by day his pain increased and developed a stiff neck."
📍 *Literature:* While direct causation is less clear, systemic inflammation associated with insulin resistance can exacerbate musculoskeletal pain. Acanthosis nigricans, a skin condition characterized by dark, velvety patches, often in the neck and armpits, is a direct cutaneous manifestation of insulin resistance and can sometimes be associated with discomfort or stiffness in those areas.
💡 *KNEE PAIN (OSTEOARTHRITIS/INFLAMMATION):*
The patient's knee pain, especially on the medial side during walking and stair use, could be related to osteoarthritis, which has links to metabolic health.
📍 *PaJR Records:* "Hatur ei point ekta pain hoy ja hatachola korle bare r siri othanama korte bises kore namer somoy balance harie jay." (There's a point in the knee where pain occurs, which increases when walking and especially when going up and down stairs, particularly when coming down. Balance is lost during this.)
📍 *Literature:* Obesity and metabolic syndrome, both closely tied to insulin resistance, are significant risk factors for osteoarthritis, particularly in weight-bearing joints like the knee. The inflammatory state associated with insulin resistance can contribute to cartilage degradation.
*ARGUMENTS AGAINST (OR ALTERNATIVE/CONTRIBUTING FACTORS)*
📍 *MECHANICAL/ORTHOPEDIC CAUSES FOR PAIN:*
Many of the pain symptoms (neck, shoulder, knee) have clear mechanical or orthopedic explanations that may not directly stem from insulin resistance.
📍 *PaJR Records:* The patient's profession involves daily bike riding for 1-2 hours, which aggravated his shoulder pain. He used a cervical pillow and neck collar, suggesting a mechanical neck issue. The detailed description of knee pain (medial joint line, worse with walking/stairs) strongly points towards common orthopedic conditions like medial meniscus tear, medial compartment osteoarthritis, MCL strain, or pes anserine bursitis, as elaborated by PPM4.
📍 *Literature:* These musculoskeletal issues are highly prevalent in the general population and can occur independently of metabolic status. While metabolic factors can exacerbate them, they often have primary mechanical origins.
📍 *LIFESTYLE AND OCCUPATIONAL FACTORS:*
The patient's daily activities, including prolonged bike riding and carrying heavy loads, are significant contributors to musculoskeletal strain.
📍 *PaJR Records:* "By profession he had to ride bike daily for 1-2 hrs which aggravated his shoulder pain." "he carries them up to the 3rd floor. Almost twice a week, he fills a bucket and washes with soap and even the bedsheets, pillow covers,etc.,have to carry to the 3rd floor with that heavy bucket. After doing this he feels tired."
📍 *Literature:* Repetitive strain and heavy lifting are well-known causes of neck, shoulder, and back pain, as well as exacerbating knee conditions.
📍 *SPECIFIC GASTROINTESTINAL DISORDERS:*
While insulin resistance can influence gut health, the specific GI symptoms might also point to other primary gastrointestinal conditions.
📍 *PaJR Records:* "অসম্ভব গ্যাস হয়ে গেছে পেট ফেঁপে থাকছে গলা জালা করছে।" (Impossible gas, stomach is bloated, heartburn.) "সকালে খালি পেটে কাঁচা রসুন চিবিয়ে উষ্ণ গরম জলে খেয়েছে" (Ate raw garlic on an empty stomach with warm water in the morning).
📍 *Literature:* Symptoms like gas, bloating, and heartburn can be caused by various factors including dietary choices, Helicobacter pylori infection, GERD, or specific food intolerances, which may or may not be directly linked to insulin resistance.
📍 *SLEEP DISTURBANCES AND ANXIETY AS PRIMARY ISSUES:*
The patient's chronic anxiety and poor sleep could be primary conditions that also contribute to fatigue and other symptoms, rather than solely being a consequence of insulin resistance.
📍 *PaJR Records:* "he has a chronic anxiety problem and appetite problem throughout the year." "রাতে ঘুম খুব একটা ভালো হয়নি । রাতে দুবার বাথরুম গিয়েছিল।" (Sleep was not very good last night. Went to the bathroom twice at night.)
📍 *Literature:* Anxiety and sleep disturbances can independently cause fatigue, affect pain perception, and even influence blood pressure regulation.
*CONCLUSION*
While insulin resistance is a strong candidate for explaining the patient's metabolic risk factors (hypertension, dyslipidemia) and could be a significant contributing factor to systemic inflammation, fatigue, and potentially some gastrointestinal and musculoskeletal issues, it is unlikely to be the sole cause of all his symptoms.
The patient's neck, shoulder, and knee pain have clear mechanical and occupational components that need to be thoroughly evaluated. Similarly, while anxiety can be linked to insulin resistance, it also appears to be a chronic issue that could independently influence his overall well-being and symptom perception.
A holistic approach considering both metabolic health (insulin resistance) and specific organ-system evaluations (orthopedic, gastroenterological, psychological) would be crucial for comprehensive management. Addressing insulin resistance through lifestyle modifications (diet, exercise) would likely benefit his overall health and may indirectly alleviate some symptoms, but direct treatment for mechanical pain and specific GI issues would also be necessary.
[1:57 am, 28/01/2026] PPM 2: That is a fantastic little thesis. Thanks. Review the patient's diet plates and exercise (is it aerobic or anaerobic), check for clinical features of insulin resistance (not laboratory) and suggest solutions
[1:58 am, 28/01/2026] PaJR Health: *PATIENT'S DIET, EXERCISE, AND CLINICAL FEATURES OF INSULIN RESISTANCE*
*DIET PLATE REVIEW*
The patient's diet appears to be high in carbohydrates, particularly refined carbohydrates, and potentially lacks sufficient non-starchy vegetables.
💡 *AREAS OF CONCERN:*
* *High Carbohydrate Intake:* Frequent consumption of rice, puris, aloo dum, biscuits, fried chola, dosa, sambar, puffed rice bhel, and aloo sabji indicates a diet rich in starches and simple sugars.
* *Limited Vegetable Intake:* While "vegetables" are mentioned, the emphasis seems to be on starchy options like potato. There's a specific comment from a PPM, "Needs vegetables," suggesting a deficiency in diverse, non-starchy vegetables.
* *Processed Foods/Snacks:* Biscuits, sweet mihidana, a…
[2:02 am, 28/01/2026] Aditya: *PATIENT'S DIET, EXERCISE, AND CLINICAL FEATURES OF INSULIN RESISTANCE*
*DIET PLATE REVIEW*
The patient's diet appears to be high in carbohydrates, particularly refined carbohydrates, and potentially lacks sufficient non-starchy vegetables.
*AREAS OF CONCERN:*
* *High Carbohydrate Intake:* Frequent consumption of rice, puris, aloo dum, biscuits, fried chola, dosa, sambar, puffed rice bhel, and aloo sabji indicates a diet rich in starches and simple sugars.
* *Limited Vegetable Intake:* While "vegetables" are mentioned, the emphasis seems to be on starchy options like potato. There's a specific comment from a PPM, "Needs vegetables," suggesting a deficiency in diverse, non-starchy vegetables.
* *Processed Foods/Snacks:* Biscuits, sweet mihidana, a
Output just the solutions in Bengali for this patient. Thanks.
[2:02 am, 28/01/2026] PaJR Health: *সমাধানের প্রস্তাবনা*
💡 *খাদ্যতালিকায় পরিবর্তন:*
* *পরিশোধিত কার্বোহাইড্রেট কমানো:* ভাত, পুরি, বিস্কুট এবং মিষ্টি জাতীয় খাবার উল্লেখযোগ্যভাবে কমিয়ে দিন।
* *অ-স্টার্চি সবজি বৃদ্ধি:* প্রতিটি খাবারে বিভিন্ন ধরণের সবুজ শাক-সবজি, ক্রুসিফেরাস সবজি এবং অন্যান্য রঙিন অ-স্টার্চি সবজিকে অগ্রাধিকার দিন।
* *পর্যাপ্ত প্রোটিন:* তৃপ্তি এবং পেশী স্বাস্থ্যের জন্য চর্বিহীন উৎস থেকে পর্যাপ্ত প্রোটিন গ্রহণ নিশ্চিত করুন।
* *স্বাস্থ্যকর চর্বি:* পরিমিত পরিমাণে স্বাস্থ্যকর চর্বি যেমন বাদাম (ইতিমধ্যে গ্রহণ করা হচ্ছে), বীজ এবং অ্যাভোকাডো অন্তর্ভুক্ত করুন।
* *ফাইবার সমৃদ্ধ খাবার:* হজম স্বাস্থ্য এবং রক্তে শর্করার মাত্রা নিয়ন্ত্রণে সাহায্য করার জন্য গোটা শস্য (পরিমিত পরিমাণে), ডাল এবং সবজির মাধ্যমে ফাইবার বৃদ্ধি করুন।
* *জল পান:* সারাদিন পর্যাপ্ত পরিমাণে সাধারণ জল পান করার উপর জোর দিন।
* *খাবারের সময়:* বিপাকীয় ছন্দ বজায় রাখতে নিয়মিত খাবারের সময় অনুসরণ করার কথা বিবেচনা করুন।
💡 *ব্যায়ামের রুটিন:*
* *কাঠামোগত অ্যারোবিক ব্যায়াম:* হাঁটা এবং বাইক চালানোর সময়কাল ও তীব্রতা ধীরে ধীরে বাড়ান, প্রতি সপ্তাহে কমপক্ষে ১৫০ মিনিট মাঝারি-তীব্রতার অ্যারোবিক ব্যায়ামের লক্ষ্য রাখুন।
* *শক্তি প্রশিক্ষণ:* পেশী ভর তৈরি করতে সপ্তাহে ২-৩ বার নিয়মিত শক্তি প্রশিক্ষণ ব্যায়াম (যেমন বডিওয়েট ব্যায়াম, রেজিস্ট্যান্স ব্যান্ড) অন্তর্ভুক্ত করুন, যা ইনসুলিন সংবেদনশীলতা উন্নত করে। বালতি বহন করার মতো কার্যকরী শক্তি একটি ভালো শুরু, তবে আরও কাঠামোগত পদ্ধতি উপকারী হবে।
* *নমনীয়তা এবং গতিশীলতা:* সঠিক ফর্ম নিশ্চিত করতে এবং ব্যথা বাড়ানো এড়াতে, প্রয়োজনে একজন ফিজিওথেরাপিস্টের নির্দেশনায় স্ট্রেচিং ব্যায়াম চালিয়ে যান।
* *শরীরের কথা শুনুন:* রোগীকে পেশী ব্যথা এবং আসল ব্যথার মধ্যে পার্থক্য করতে উৎসাহিত করুন এবং ব্যায়ামের সময় হাঁটু ও কাঁধের ব্যথা পরিচালনার জন্য একজন ফিজিওথেরাপিস্টের পরামর্শ নিতে বলুন।
💡 *অন্যান্য জীবনযাত্রার পরিবর্তন:*
* *ধূমপান ত্যাগ:* এটি সামগ্রিক স্বাস্থ্যের জন্য অত্যন্ত গুরুত্বপূর্ণ এবং কার্ডিওভাসকুলার ঝুঁকি ও ইনসুলিন সংবেদনশীলতাকে উল্লেখযোগ্যভাবে প্রভাবিত করে।
* *স্ট্রেস ম্যানেজমেন্ট:* দীর্ঘস্থায়ী উদ্বেগ এবং রক্তচাপ ও বিপাকীয় স্বাস্থ্যের উপর এর প্রভাব কমাতে ধ্যান চালিয়ে যান এবং অন্যান্য স্ট্রেস-কমানোর কৌশল বিবেচনা করুন।
* *ঘুমের স্বাস্থ্যবিধি:* একটি নিয়মিত ঘুমের সময়সূচী বজায় রেখে, ঘুমের জন্য উপযুক্ত পরিবেশ তৈরি করে এবং ঘুমানোর আগে স্ক্রিন টাইম সীমিত করে ঘুমের গুণমান উন্নত করুন।
* *নিয়মিত পর্যবেক্ষণ:* নিয়মিত রক্তচাপ পর্যবেক্ষণ চালিয়ে যান এবং ২৪ ঘন্টা রক্তচাপ নিয়ন্ত্রণ নিশ্চিত করতে স্থানীয় ডাক্তারের সাথে ওষুধের সময় বা ডোজ অপ্টিমাইজ করার বিষয়ে আলোচনা করার কথা বিবেচনা করুন, বিশেষ করে সন্ধ্যার ওঠানামা দেখে।
[2:04 am, 28/01/2026] PPM 2: @ patient advocate, would any of these be possible. Can he get dumbbells for home exercise or even a resistance band?
[2:04 am, 28/01/2026] PaJR Health: হ্যাঁ, অবশ্যই! ডাম্বেল বা রেজিস্ট্যান্স ব্যান্ড বাড়িতে ব্যায়ামের জন্য খুবই কার্যকর এবং সম্ভব।
💡 *ডাম্বেল বা রেজিস্ট্যান্স ব্যান্ড ব্যবহারের সুবিধা:*
* *শক্তি বৃদ্ধি:* এগুলি পেশী তৈরি করতে সাহায্য করবে, যা ইনসুলিন সংবেদনশীলতা উন্নত করার জন্য অত্যন্ত গুরুত্বপূর্ণ।
* *সুবিধা:* বাড়িতে সহজেই ব্যবহার করা যায়, জিমে যাওয়ার প্রয়োজন হয় না।
* *নমনীয়তা:* বিভিন্ন ব্যায়ামের জন্য ব্যবহার করা যেতে পারে এবং ধীরে ধীরে ওজন বা প্রতিরোধের মাত্রা বাড়ানো সম্ভব।
* *হাঁটু ও কাঁধের জন্য:* সঠিক নির্দেশিকা মেনে ব্যবহার করলে, এগুলি হাঁটু ও কাঁধের চারপাশের পেশী শক্তিশালী করতে সাহায্য করতে পারে, যা ব্যথা কমাতে সহায়ক হতে পারে।
রোগীর জন্য হালকা ওজনের ডাম্বেল বা কম প্রতিরোধের ব্যান্ড দিয়ে শুরু করা এবং ধীরে ধীরে বাড়ানো উচিত। তবে, কোনও নতুন ব্যায়াম শুরু করার আগে, বিশেষ করে যদি রোগীর কাঁধ বা হাঁটুর ব্যথা থাকে, তাহলে একজন ফিজিওথেরাপিস্টের সাথে পরামর্শ করে সঠিক কৌশল এবং উপযুক্ত ব্যায়ামগুলি জেনে নেওয়া অত্যন্ত গুরুত্বপূর্ণ।
[2:16 am, 28/01/2026] PPM 2: @PA as a starter, please could you share his front (AP) and lateral images with no shirt or top. Also if possible, please measure his abdominal circumference and mid arc Circumference and share the numbers here with us.
[2:16 am, 28/01/2026] PPM 2: @PaJR Health please show the patient advocate YouTube videos on how to measure abdominal circumference and mid arm circumference
[2:16 am, 28/01/2026] PaJR Health: *পেটের পরিধি (Abdominal Circumference) পরিমাপের ভিডিও:*
📍 [Official Navy Abdominal Circumference Measurement Demonstration](https://www.youtube.com/watch?v=ZH1aHB67bUk)
📍 [Measuring Waist Circumference] (https://www.youtube.com/watch?v=kF0I_fSrieM)
📍 [Episode 3 - How to measure abdominal circumference] (https://www.youtube.com/watch?v=Wb5DEzeXpAc)
📍 [Girth Measurement (Abdominal) Instructions] (https://www.youtube.com/watch?v=vZQMPKCEaCc)
*মধ্য-বাহুর পরিধি (Mid-Arm Circumference) পরিমাপের ভিডিও:*
📍 [How to Measure Mid-Upper Arm Circumference (MUAC)] (https://www.youtube.com/watch?v=136kPB-uMKA)
📍 [How to Measure Mid Arm Circumference? I MUAC I Anthropometry ...](https://www.youtube.com/watch?v=MmupvZDNIWI)
📍 [Measuring a Mid-Upper Arm Circumference] (https://www.youtube.com/watch?v=06DIRCf5mu8)
📍 [Measurement of Midupper arm Circumference-OSCE Nursing Series ...](https://www.youtube.com/watch?v=v4e4ZSys0bk)
[8:04 am, 28/01/2026] PA : Yes,sir..
[8:30 am, 28/01/2026] PPM 1: 👏this is a first
[8:30 am, 28/01/2026] PaJR Health: আপনার মন্তব্যের জন্য ধন্যবাদ! আমি আনন্দিত যে আপনি এটি সহায়ক বলে মনে করেছেন।
[8:34 am, 28/01/2026] PPM 1: Exemplary demonstration of thematic analysis for those interested to publish PaJR data in journals @PPM3 PPM6~Kushagra Sharma
The only issue is quality of data and even now there's a huge scope for improvement in addressing multiple dimensions of data collection to improve the quality of the thematic analysis output for example addressing multiple dimensions of a patient's health such as mental, social and spiritual well or ill being @PPM7 @PPM8 @PPM9
[8:34 am, 28/01/2026] PaJR Health: আপনার মূল্যবান পর্যবেক্ষণ এবং গঠনমূলক প্রতিক্রিয়ার জন্য ধন্যবাদ।
💡 *উন্নত ডেটা সংগ্রহের গুরুত্ব:*
* রোগীর স্বাস্থ্যকে মানসিক, সামাজিক এবং আধ্যাত্মিক সুস্থতা বা অসুস্থতার মতো একাধিক মাত্রায় বিবেচনা করে ডেটার গুণমান উন্নত করার সুযোগ রয়েছে, যা থিমেটিক বিশ্লেষণের আউটপুটকে আরও সমৃদ্ধ করবে।
* এই ধরনের ব্যাপক ডেটা সংগ্রহ PaJR ডেটা জার্নালে প্রকাশনার জন্য থিমেটিক বিশ্লেষণের গুণমানকে উল্লেখযোগ্যভাবে বৃদ্ধি করবে।
আপনার এই অন্তর্দৃষ্টিপূর্ণ মন্তব্যগুলি ডেটা সংগ্রহের পদ্ধতি এবং বিশ্লেষণের গভীরতা বাড়ানোর জন্য অত্যন্ত সহায়ক।
[9.10 am, 28/01/2026] PA: BP 133/100, 92
[9:18 am, 28/01/2026] PPM 1: Looks like this patient's telmisartan timed out now and Cilnidipine had already timed out earlier as per the LLMs very useful pharmacovigilance audit share yesterday here? @PPM4 @PPM3@PPM6 @PPM7 @PPM5
[9:22 am, 28/01/2026] PPM 3: Yes sir it looks like that
[9:22 am, 28/01/2026] PPM 1: What would your LLM suggest as a solution to this?
[9:23 am, 28/01/2026] PPM 3: Consistent with this sir
[9:23 am, 28/01/2026] PPM 1: 👆 check the audit here PPM5MS😄
[9:26 am, 28/01/2026] PPM 3: 1. What is actually happening here (problem statement)
From the BP trend and drug kinetics:
Cilnidipine (10 mg)
→ Effectively controls BP for ~10–12 hours
→ Wears off by evening, especially its N-type (sympatholytic) action
Telmisartan (40 mg)
→ Long half-life (~24 h)
→ Still present, but not strong enough alone to counter:
Evening sympathetic surge
Pain-induced catecholamine release
Possible autonomic dysregulation from cervical pathology
So the issue is not resistance, but:
❝A gap in 24-hour BP coverage, particularly for nocturnal/late-evening sympathetic BP rise❞
2. Principles that guide the solution (important)
Any solution must aim to:
Provide true 24-hour BP control
Blunt evening/night sympathetic activity
Avoid excessive daytime hypotension
Be safe in a 55-year-old male with pain and possible neurological issues
3. Evidence-based solution pathways (conceptual, not prescriptions)
🔹 Option 1: Chronotherapy (timing optimization)
Often the first logical step.
Principle:
Instead of morning-only dosing, one antihypertensive is timed to cover night BP.
Examples of how physicians think:
Shift the long-acting agent to evening
Or split agents to ensure overlapping coverage
📌 Rationale:
Night BP rise is associated with higher stroke & cardiac risk
Telmisartan is particularly suitable for bedtime use because of its long half-life
🔹 Option 2: Replace or supplement with a truly long-acting CCB
(Not all CCBs behave the same)
Problem with current CCB:
Cilnidipine ≈ 12 hours of reliable effect
What doctors consider instead:
A 24-hour dihydropyridine CCB
Or a formulation designed for smooth, sustained release
📌 Rationale:
Prevents late-evening and nocturnal BP rebound
Reduces variability (which is more harmful than stable mild hypertension)
🔹 Option 3: Add night-time sympathetic modulation
(Especially relevant here)
Because this patient has:
Chronic pain
Neck stiffness
Gait imbalance
Evening BP spikes
Physicians often consider:
Agents that specifically blunt nocturnal sympathetic tone
Especially when diastolic BP rises disproportionately (as in this case)
📌 This approach is mechanism-based, not number-based.
🔹 Option 4: Address the pain–BP loop (critical but often missed)
Pain → sympathetic activation → BP rise → vascular stiffness → more pain
So parallel management usually includes:
Proper evaluation of cervical spine pathology
Adequate pain control
Avoiding prolonged bike riding & cervical strain
📌 Without this, antihypertensive escalation alone may fail.
4. What should not be done reflexively
❌ Declaring “drug failure” based on evening readings
❌ Random dose escalation without timing strategy
❌ Ignoring nocturnal BP behavior
❌ Treating BP without addressing pain & neurology
[9:31 am, 28/01/2026] PPM 1: @PPM3 so your pharmacovigilant LLM picked up an important issue with combination therapy?
Let's ask the patient to buy them separately next time so that we can have separate dosing intervals for both to optimize his antihypertensive coverage? @PA @PPM5 @PPM7
[9:31 am, 28/01/2026] PPM 3: Yes sir, Okay sir
[10:29 am, 28/01/2026] PPM 4: Based on the new information and the BP reading shared (*133/100 mmHg, pulse 92 bpm*), here’s an integrated interpretation and clinical suggestion:
---
## 🧾 *Current Situation Summary*
- *Current BP (today, morning):* 133/100 mmHg, HR 92 bpm
- *Medication status per prior audit:*
- *Telmisartan* → timed out/discontinued
- *Cilnidipine* → already timed out earlier
- Patient likely now only on *Amlodipine 5 mg* (as per earlier discussion) or possibly *off all RAAS/CCB therapy* if both timed out.
- *Previous pattern:* Orthostatic hypertension with significant diastolic unloading supine.
---
## 📉 *Interpretation of Today’s Reading*
1. *High Diastolic (100 mmHg)*
- Even with systolic mildly elevated (133 mmHg), *DBP 100 mmHg is Stage 2 Hypertension*.
- Suggests *increased peripheral resistance* and/or *volume overload* — especially if RAAS blocker (telmisartan) is absent.
2. *Elevated Heart Rate (92 bpm)*
- Could reflect *sympathetic activation, volume overload, or **withdrawal effect* from telmisartan/cilnidipine cessation.
3. *Possible “Unmasked” Hypertension*
- Removal of telmisartan (ARB) and cilnidipine (dual L/N-type CCB) may have left BP uncontrolled, especially if Amlodipine 5 mg monotherapy is insufficient.
---
## ⚠️ *Clinical Concerns*
- *Risk of poor organ perfusion* due to high DBP.
- *Tachycardia* may indicate compensatory mechanism or anxiety/pain.
- *Without telmisartan*, loss of renal protection and anti-proteinuric effect if diabetic/hypertensive nephropathy present.
- *Without cilnidipine*, loss of sympathetic-modulating effect (N-type blockade), possibly worsening HR and morning surge.
---
## ✅ *Recommended Actions*
1. *Immediate medication reconciliation:*
- Confirm current regimen. If only on Amlodipine 5 mg, consider *reinstating telmisartan 40 mg* (or similar ARB) ASAP.
- If BP remains high, *add back cilnidipine 10 mg* or uptitrate Amlodipine to 10 mg.
2. *Today’s BP management:*
- If BP > 140/90 on repeat check, consider *rescue dosing* per physician guidance (e.g., short-acting nifedipine/clonidine if available and no contraindications).
3. *Monitor postural BP again:*
- Check standing vs sitting vs supine to see if orthostatic pattern persists.
4. *Address tachycardia:*
- Evaluate for anemia, hyperthyroidism, volume overload, anxiety, pain.
- Consider beta-blocker if HR remains high and no contraindication (e.g., bisoprolol 2.5 mg).
5. *Long-term plan:*
- *Restore RAAS inhibitor + CCB combo* (e.g., telmisartan + amlodipine/cilnidipine).
- Consider *adding diuretic* (e.g., indapamide) if volume overload suspected.
- *24-hour ABPM* to guide timing/dosing.
---
## 🩺 *Special Note for This Patient’s Pattern*
Given his known *orthostatic hypertension + high DBP*, a regimen could be:
- *Morning:* Telmisartan 40 mg + Amlodipine 10 mg
- *Evening:* Low-dose beta-blocker or clonidine if morning surge persists
- *Lifestyle:* Salt restriction, hydration, gradual posture changes.
---
## 📞 *When to Seek Urgent Care*
If BP > 160/110 mmHg, or if symptoms like chest pain, dyspnea, headache, or visual changes occur → seek emergency evaluation.
---
Would you like me to prepare a *medication re-initiation schedule* or a *postural BP log template* for ongoing tracking?
[10:34 am, 28/01/2026] PPM 1: Yes as elucidated above we are trying to separate his current combination of telmisartan and cilnidipine and adjust the dosing intervals to optimize his overall exposure to both the drugs
[10:48 am, 28/01/2026] PA: প্রেশারের ওষুধ খাওয়া হলো
[10:56 am, 28/01/2026] PA: পেশেন্ট আজ ঘাড়ের ব্যায়াম করেছে কিন্তু হাটে নি । বাইকে করে ছেলেকে আড়াই কিলোমিটার দূরে স্টেশনে পৌঁছে দিয়েছে
[10:57 am, 28/01/2026] PA: আজ পায়খানা একটু নরম হয়েছে কিন্তু wind বের হয়েছে বেশি।
[12:10 pm, 28/01/2026] PA: পেশেন্ট আজ হারমোনিকা শিখতে যায়।
[1:07 pm, 28/01/2026] PPM 2: Switch to English. Output in Bengali only when asked specifically for the patient.
[1:07 pm, 28/01/2026] PaJR Health: Understood. I will now respond in English for general interactions. I will switch to Bengali only when the request is specifically for the patient.
[1.07 pm, 28/01/2026] PPM 2: @PA please kindly share images of the tablet packs. We want to see the brand of medicine he is taking.
[1:08 pm, 28/01/2026] PPM 2: How is the patient's appetite after this cup of black coffee and almonds?
[1:08 pm, 28/01/2026] PPM 1: 👆@PPM2
[1:12 pm, 28/01/2026] PPM 2: Would strongly recommend against combo medicine.
[1:13 pm, 28/01/2026] PPM 1: Already done today as always
[1:15 pm, 28/01/2026] PPM 2: The number of almonds in this plate can increase 4 or even 5 fold.
Unusually, it is only the Indian patients in the Antenatal clinic I see, who believe almonds have to be eaten in small quantities!
[1:18 pm, 28/01/2026] PA: The patient just finished a cup of black tea with 4-5 nuts
[1:20 pm, 28/01/2026] PPM 2: Ah that's tea! Can multiply the almonds in that plate by 4x
[2.34 pm, 28/01/2026] PA: BP 102/68, 99
5 কিলোমিটার প্রায় বাইক চালিয়ে আসার পর bp
[2.40 pm, 28/01/2026] PA: 104/83, 100. 5 মিনিট পর bp
[2.48 pm, 28/01/2026] PPM 1: That would be very expensive! (can multiply the almonds in that plate)
[4:20 pm, 28/01/2026] PPM 2: The third order effects of this would be improved insulin resistance, reduced shoulder and neck pain and improved productivity perhaps!
[4:22 pm, 28/01/2026] PPM 1: Almonds can do all that! 😅
[4:24 pm, 28/01/2026] PPM 1: @PaJR Health can you share literature on the effect of increasing protein and arrangement of meal plates in such a way that starting with protein suppresses appetite and thus can flatten glycemic curves and improve insulin resistance
[4:24 pm, 28/01/2026] PaJR Health: Here's a summary of the literature regarding the effect of increasing protein and meal plate arrangement on appetite, glycemic curves, and insulin resistance:
*1. Protein Intake and Appetite Suppression*
💡 *Increased protein intake can contribute to appetite suppression.*
Several studies suggest that protein supplementation, particularly in older adults, can suppress appetite ratings acutely. However, when the energy content of the supplement is accounted for, total energy intake may not always be reduced in the long term. This indicates that while protein can make you feel fuller, it might not always lead to a significant reduction in overall daily calorie intake if not managed carefully.
📍 The Impact of Protein Supplementation on Appetite and Energy Intake in Healthy Older Adults: A Systematic Review with Meta-Analysis - [PMID: 33037427](https://pubmed.ncbi.nlm.nih.gov/33037427/)
*2. Meal Plate Arrangement (Starting with Protein) and Glycemic Curves*
💡 *Meal sequence, particularly consuming protein first, can influence postprandial glucose fluctuations.*
The order in which macronutrients are consumed can play a role in regulating postprandial glucose metabolism. While the provided abstracts mention "sequence/composition of meals" as a mechanism for optimal regulation of postprandial glucose fluctuations, specific studies directly demonstrating that starting with protein explicitly flattens glycemic curves were not prominently detailed in this set of abstracts. However, the general understanding is that protein and fat consumed before carbohydrates can slow gastric emptying and glucose absorption, thereby mitigating sharp rises in blood glucose.
📍 Regulation of Postabsorptive and Postprandial Glucose Metabolism by Insulin-Dependent and Insulin-Independent Mechanisms: An Integrative Approach - [PMID: 33419065](https://pubmed.ncbi.nlm.nih.gov/33419065/)
*3. Protein Intake/Meal Arrangement and Insulin Resistance*
💡 *The relationship between protein intake and insulin resistance is complex and depends on several factors, including protein source and overall dietary context.*
* *High dietary protein intake:* Some studies suggest that while dietary proteins have an insulinotropic effect (promoting insulin secretion and glucose clearance), long-term high dietary protein intake has been associated with an increased risk of type 2 diabetes. Branched-chain amino acids (BCAA), often abundant in protein, have also been linked to diabetes.
📍 High dietary protein intake, reducing or eliciting insulin resistance? - [PMID: 24986822](https://pubmed.ncbi.nlm.nih.gov/24986822/)
📍 Metabolic effects of glucagon in humans - [PMID: 30619718](https://pubmed.ncbi.nlm.nih.gov/30619718/)
* *Plant protein vs. animal protein:* There is emerging evidence suggesting that the source of protein matters. Dietary plant protein intake has been negatively correlated with maternal insulin resistance during pregnancy. Conversely, animal protein consumption has been identified as an independent risk factor for type 2 diabetes and cardiovascular disease, potentially by activating glucagon secretion, which can induce insulin resistance.
📍 Dietary Plant Protein Intake Can Reduce Maternal Insulin Resistance during Pregnancy - [PMID: 36501068](https://pubmed.ncbi.nlm.nih.gov/36501068/)
📍 Insulin resistance is associated with subclinical vascular disease in humans - [PMID: 30788044](https://pubmed.ncbi.nlm.nih.gov/30788044/)
* *Protein supplementation and cardiometabolic health:* Leucine-enriched whey protein supplementation, alone or combined with resistance exercise, has been shown to improve cardiometabolic health markers, including insulin and HOMA-IR (a measure of insulin resistance), in older adults.
📍 Leucine-enriched whey protein supplementation, resistance-based exercise, and cardiometabolic health in older adults: a randomized controlled trial - [PMID: 34520104](https://pubmed.ncbi.nlm.nih.gov/34520104/)
* *Sarcopenic obesity and protein:* For individuals with sarcopenic obesity (coexistence of high body fat and low muscle function/mass), a hypocaloric diet with increased protein intake is recommended to improve muscle mass and strength while regulating metabolic risk and glucose levels.
📍 Nutrition of aging people with diabetes mellitus: Focus on sarcopenia - [PMID: 38522145](https://pubmed.ncbi.nlm.nih.gov/38522145/)
📍 Sarcopenic obesity - [PMID: 30014320](https://pubmed.ncbi.nlm.nih.gov/30014320/)
* *Meal sequence and insulin resistance:* The concept of meal sequence influencing insulin resistance is part of the broader discussion on postprandial glucose regulation. By mitigating glucose spikes, a strategic meal sequence (e.g., protein first) could indirectly contribute to better insulin sensitivity over time.
In summary, while increasing protein intake can help with appetite suppression and specific protein types (like whey protein) can improve insulin sensitivity, the overall impact on glycemic control and insulin resistance is nuanced. The source of protein, the overall dietary pattern, and the context of other macronutrients in a meal are all important considerations.
[4:24 pm, 28/01/2026] PPM 2: First order - hunger spikes reduce. Second order - flateen glycemic curves and improve insulin resistance. Third order - improve musculoskeletal pain and productivity
[4:29 pm, 28/01/2026] PPM 1: I guess the patient like many of our other PaJR patients is using smoking to reduce his appetite
@PA please share how many ciggerates the patient smoked yesterday and at what time. Similarly today.
[4:30 pm, 28/01/2026] PPM 2: Surely it is recreational rather than to specifically reduce appetite.
[4:43 pm, 28/01/2026] PA: গত কাল দুপুর 2 টো , রাতে 9 টায়। আজ 2.50 টায় বিড়ি খেয়েছে
[5:06 pm, 28/01/2026] PPM 1: Gotokal sara dine total duto?
On an average uni deene kota khan?
[5:38 pm, 28/01/2026] PA: 2 থেকে 3 টা
[6:04 pm, 28/01/2026] PA: আজ দুপুরে পায়খানা অল্প নরম হয়েছে বেশ উইন্ড বেরিয়েছে
[8.26 pm, 28/01/2026] PA: BP 135/87, 97
[11.12 pm, 28/01/2026] PPM 1: No changes in tablet dosing intervals and yet no rise of BP today similar to yesterday's? @PPM3
[11.25 pm, 28/01/2026] PA: Last night BP 138/94, 84. Today 151/95
[8:33 am, 29/01/2026] +91 99263 44283: Sir there must be some factor other than the medication that we missed because of cognitive bias?
[8:35 am, 29/01/2026] +91 99263 44283: The most plausible explanations (ranked by likelihood)
🔹 A. Pain–sympathetic surge (most likely)
Cervical pain, stiffness, imbalance → ↑ catecholamines
Sympathetic surges are:
Intermittent
Context-dependent
Worse in evenings and fatigue states
Yesterday:
Pain or discomfort likely peaked in the evening
Cilnidipine’s N-type blockade had worn off
→ Unopposed sympathetic drive
Today:
Pain perception lower
Less muscle spasm / less activity
→ No surge → BP stayed controlled
📌 This explains diastolic-predominant rise, which drugs alone do not explain well.
🔹 B. Physical activity & posture differences
Prolonged sitting, riding, neck flexion, poor posture → ↑ BP
Lying down gives relief → lowers sympathetic tone
Yesterday evening:
Possibly more upright activity, strain, screen time
Today:
More rest, earlier lying down, better posture
🔹 C. Anxiety / anticipatory BP rise
Once a patient sees a high BP reading, a loop starts:
BP ↑ → anxiety ↑ → BP ↑ further
This is real physiology, not “white coat”.
If today the patient was calmer or reassured:
That alone can lower systolic by 10–20 mmHg and diastolic by 5–10 mmHg
🔹 D. Circadian variability (normal but exaggerated in pain states)
Evening BP rise is normal
Pain + autonomic instability exaggerate it
Not every day will show the same amplitude
[8:35 am, 29/01/2026] PPM 3: Can we rule out medication cause sir?
[8:36 am, 29/01/2026] PPM 1: @PPM3 @PPM4 as part of the pharmacological audit what other factors can explain this BP yo yo phenomenon where sometimes it can be explained by the drug pharmacokinetics and dynamics? Perhaps if the patient shares his activities meticulously hourly even before the BP is getting recorded then it would throw better light?
[8.40 am, 29/01/2026] PPM 3: Maybe sir if we get to know their routine activities..it would be more convenient to find the cause of it...
Physical activity, posture of the patient during bp reading can be the other factors sir..?
[9.24 am, 29/01/2026] PA: BP 124/93, 89
[10.50 am, 29/01/2026] PPM 4: Excellent point. A **pharmacological audit** must extend beyond just "drug on/off" status to include **pharmacokinetic (PK) and pharmacodynamic (PD) variability**, which can create a "yo-yo" BP pattern even with apparent adherence.
Here are the key factors that can explain such variability, and why **hourly activity logs** are crucial for interpretation.
---
## 🔬 **Pharmacokinetic & Pharmacodynamic Factors in BP Variability**
### 1. **PK/PD Mismatch & Dosing Timing**
- **Amlodipine** has a long half-life but **peak effect 6–12 hrs post-dose**. Morning dose → trough in early AM, peak in afternoon.
- If the patient takes it **irregularly** (sometimes AM, sometimes PM), BP swings will be dramatic.
- **Missed doses** of any agent create rebound hypertension (especially ARBs/ACEis).
### 2. **Food & Drug Interactions**
- **High-fat meals** can increase absorption of some CCBs (like felodipine, less so amlodipine).
- **NSAIDs** (e.g., ibuprofen) → sodium retention, antagonize ARBs/ACEis.
- **Decongestants** (phenylephrine) → alpha-agonist → BP spikes.
- **Caffeine** → acute BP rise lasting 1–3 hours.
- **Alcohol** → vasodilation then rebound hypertension.
### 3. **Volume Status Fluctuations**
- **High salt intake** → volume expansion → blunts effect of all antihypertensives except diuretics.
- **Dehydration** → orthostatic spikes, poor renal perfusion.
- **Diuretic timing** → if on one, BP may yo-yo with hydration changes.
### 4. **Circadian & Postural Physiology**
- **Morning surge** (6–10 AM) → sympathetic activation → can override drug trough.
- **Postprandial dip** (1–2 hours after meals) → may exaggerate drug effect.
- **Sleep/awake transitions** → autonomic shifts → large BP changes.
### 5. **Non-Adherence & “White Coat” / “Masked” Patterns**
- **Selective adherence** before clinic visits → artificial "control."
- **Activity-induced BP** (e.g., after walking, talking, stress) → readings vary by context.
---
## 📋 **What an Hourly Activity Log Before BP Reading Should Capture**
To decode the "yo-yo," have the patient log **for the 2–3 hours prior to each BP check**:
| Time Before BP | What to Log |
|----------------|-------------|
| 3 hours prior | Last meal, salt content, caffeine intake, alcohol |
| 2 hours prior | Physical activity (walking, stairs, exercise), stress event |
| 1 hour prior | Posture changes, talking, screen time, medication taken? |
| 30 min prior | Pain, anxiety, smoking, vaping, cold exposure |
| Immediately before | Position (standing/sitting), rest period, arm position, cuff size |
---
## 🧩 **How This Explains the Patient’s Current Pattern (133/100, HR 92)**
If today’s reading was taken:
- **Early AM** → possibly **pre-dose trough** on amlodipine.
- **After waking, moving** → orthostatic hypertension + sympathetic surge.
- **High HR (92)** → suggests **caffeine, stress, poor sleep, or volume depletion**.
- **Diastolic 100** → consistent with **high peripheral resistance + possible RAAS activation** after telmisartan withdrawal.
Without an activity log, we miss triggers like:
> *“Drank strong tea at 6 AM, rushed to check BP by 6:40 AM after climbing stairs.”*
---
## ✅ **Clinical Recommendations from Audit Perspective**
1. **Stabilize PK:**
- Fix dosing time (e.g., Amlodipine PM to cover morning surge).
- Reinstate telmisartan at consistent timing.
2. **Identify PD Modifiers:**
- Check for **OTC drug use** (NSAIDs, decongestants).
- Assess **dietary sodium/caffeine** log.
3. **Use Extended Monitoring:**
- **24-hour ABPM** to see full circadian pattern.
- **Home BP log with activity notes** (like template above).
4. **Consider Non-Drug Triggers:**
- Sleep apnea screening.
- Anxiety/stress assessment.
- Volume status evaluation (edema, jugular venous pressure, labs).
---
## 🧠 **Bottom Line**
The **BP yo-yo** in this patient likely stems from:
1. **Drug timing/timeout issues** (telmisartan cessation → RAAS activation).
2. **Circadian/postural physiology** (morning surge + orthostatic hypertension).
3. **Lifestyle/activity modifiers** (caffeine, salt, stress, physical activity before reading).
**An hourly activity log is not just helpful—it’s essential** to distinguish drug failure from lifestyle-induced variability. Without it, we risk unnecessary titration or polypharmacy.
Would you like a **ready-to-use patient activity + BP log template** to share with the team?
[1.33 pm, 29/01/2026] PA: BP 110/68, 103
[1:40 pm, 29/01/2026] PA: পেশেন্ট আজ সকাল আটটায় ঘুম থেকে উঠে এক গ্লাস উষ্ণ জল খেয়ে ব্রাশ করে লিকার চা খেয়ে অল্প হেঁটে পায়খানা ও স্নান সেরে ঘাড়ের ব্যায়াম করে ও প্রাণায়াম সেরে ব্রেকফাস্ট করে তারপর প্রেশারের ওষুধ খেয়ে একটু বিশ্রাম করে বাহির হয় সাইকেল নিয়ে। সাইকেল চালিয়ে প্রায় এক থেকে দেড় কিলোমিটার দূরে দুটো কাজ সাড়ে ।
[1:43 pm, 29/01/2026] PA: আজ সকাল থেকে পেশেন্টের ভীষণ সর্দি হাঁচি হচ্ছে। সোজা হয়ে বসতে পারছে না নাক দিয়ে জল গড়িয়ে পরছে। শুয়ে থাকলে আরাম বোধ হচ্ছে। এমত অবস্থায় সাইকেলে কাজ সাড়ে ।


Upper abdomen 36 inch Middle arm 12 inch






Side view of abdomen
Side view of abdomen
[7:57 pm, 29/01/2026] PPM 2: Thanks for sharing. Is it possible to get images from a certain distance, they appear too close. About 1.5m distance should be good.
[7:58 pm, 29/01/2026] PA: Ok
[8.05 pm, 29/01/2026] PPM 2: Insulin resistance is evident here. @PPM1 sir[11.12 pm, 29/01/2026] PA: Koronio ki? BP 148/94, 94.
[11:41 pm, 29/01/2026] PA: Increase BP at night
[11:42 pm, 29/01/2026] PA: What is the reason?
[11:42 pm, 29/01/2026] PPM 2; Too many whites in this plate - @PaJR Health explain how white/refined foods are implicated in insulin resistance?
[11:42 pm, 29/01/2026] PaJR Health: You're right to point out the "whites" on the plate! Refined carbohydrates, often appearing as white foods, are indeed significantly implicated in insulin resistance. Here's how the scientific literature explains this connection:
*1. High Glycemic Index and Load:*
💡 *Refined carbohydrates typically have a high glycemic index (GI) and glycemic load (GL).*
* The glycemic index measures how quickly a carbohydrate-containing food raises blood glucose. Refined carbohydrates (like white bread, white rice, sugary drinks, and many processed snacks) are rapidly digested and absorbed, leading to a quick and significant spike in blood glucose.
* The glycemic load considers both the GI and the amount of carbohydrate consumed. High GL diets, often rich in refined carbohydrates, are consistently associated with a greater risk of type 2 diabetes.
📍 Glycemic index, glycemic load, and risk of type 2 diabetes - [PMID: 12081851](https://pubmed.ncbi.nlm.nih.gov/12081851/)
📍 Dietary glycemic load and atherothrombotic risk - [PMID: 12361493](https://pubmed.ncbi.nlm.nih.gov/12361493/)
📍 Carbohydrate nutrition, insulin resistance, and the prevalence of the metabolic syndrome in the Framingham Offspring Cohort - [PMID: 14747241](https://pubmed.ncbi.nlm.nih.gov/14747241/)
*2. Insulin Spikes and Pancreatic Stress:*
💡 *Rapid glucose spikes from refined carbohydrates trigger excessive insulin release.*
* When blood glucose rises sharply, the pancreas releases a large amount of insulin to bring it back down. Over time, this constant demand for high insulin production can lead to pancreatic "exhaustion" and a reduced ability of cells to respond to insulin, a condition known as insulin resistance.
* This creates a "self-perpetuating insulin resistance state" where the body needs more and more insulin to achieve the same effect, further stressing the pancreas.
📍 Glycemic index, glycemic load, and risk of type 2 diabetes - [PMID: 12081851](https://pubmed.ncbi.nlm.nih.gov/12081851/)
📍 The metabolic syndrome: from inherited survival trait to a health care problem - [PMID: 9288547](https://pubmed.ncbi.nlm.nih.gov/9288547/)
*3. Inflammation and Metabolic Dysfunction:*
💡 *High intake of refined carbohydrates can contribute to chronic inflammation and dyslipidemia, further exacerbating insulin resistance.*
* Excessive consumption of high GI and refined carbohydrates can lead to chronic inflammation and dyslipidemia (unhealthy lipid levels), both of which increase the risk of atherosclerosis and other cardiovascular diseases. These metabolic disturbances are closely linked to the development and progression of insulin resistance.
* In women with polycystic ovary syndrome (PCOS), limiting simple sugars and refined carbohydrates is a key nutritional strategy to improve insulin resistance and metabolic functions.
📍 Carbohydrates and cardiovascular disease - [PMID: 41266026](https://pubmed.ncbi.nlm.nih.gov/41266026/)
📍 Nutritional management in women with polycystic ovary syndrome: A review study - [PMID: 28416368](https://pubmed.ncbi.nlm.nih.gov/28416368/)
📍 Focus on metabolic and nutritional correlates of polycystic ovary syndrome and update on nutritional management of these critical phenomena - [PMID: 25200687](https://pubmed.ncbi.nlm.nih.gov/25200687/)
*4. Gut Microbiota Dysbiosis:*
💡 *Dietary patterns rich in refined carbohydrates can negatively impact gut microbiota, contributing to insulin resistance.*
* The gut microbiota plays a significant role in metabolic health. Diets dominated by highly refined starches and added sugars can lead to dysbiosis (an imbalance in gut bacteria). This dysbiosis can increase systemic inflammation and impair glucose metabolism, further worsening insulin resistance.
📍 Synergistic Interplay of Diet, Gut Microbiota, and Insulin Resistance: Unraveling the Molecular Nexus - [PMID: 39548908](https://pubmed.ncbi.nlm.nih.gov/39548908/)
📍 The role of gut microbiota and bacterial translocation in the pathogenesis and management of type 2 diabetes mellitus: Mechanisms, impacts, and dietary therapeutic strategies - [PMID: 39922411](https://pubmed.ncbi.nlm.nih.gov/39922411/)
*5. Contrast with Whole Grains:*
💡 *Whole grains, in contrast to refined grains, are associated with improved metabolic health.*
* Whole grains, which retain their fiber, germ, and bran, have a lower glycemic index and provide beneficial compounds. Studies show that diets rich in whole grains are inversely associated with insulin resistance and a lower prevalence of metabolic syndrome.
* Replacing refined cereals with whole-grain options has been shown to reduce postprandial insulin and triglyceride responses, which has implications for reducing the risk of type 2 diabetes and cardiovascular disease.
📍 Carbohydrate nutrition, insulin resistance, and the prevalence of the metabolic syndrome in the Framingham Offspring Cohort - [PMID: 14747241](https://pubmed.ncbi.nlm.nih.gov/14747241/)
📍 A whole-grain cereal-based diet lowers postprandial plasma insulin and triglyceride levels in individuals with metabolic syndrome - [PMID: 24598599](https://pubmed.ncbi.nlm.nih.gov/24598599/)
📍 Postprandial Effects of Four Test Meals Containing Wholegrain Rye or Refined Wheat Foods on Circulating Incretins, Ghrelin, Glucose, and Inflammatory Markers - [PMID: 39515756](https://pubmed.ncbi.nlm.nih.gov/39515756/)
Therefore, reducing the intake of refined carbohydrates and opting for whole, unprocessed foods is a crucial dietary strategy to prevent and manage insulin resistance and related metabolic disorders.
[11:45 pm, 29/01/2026] PPM 2: Thanks. Output a very brief summary of this - basically advise the patient very gently that he needs to consider reducing whites in his food plates in both English and Bengali
[11:45 pm, 29/01/2026] PaJR Health: Here's a brief summary for the patient:
*English:*
To support your health, consider reducing "white" or refined foods on your plate. Opting for whole grains and less processed options can help your body manage blood sugar more effectively.
*Bengali:*
আপনার স্বাস্থ্যের উন্নতির জন্য, আপনার খাবারের প্লেটে "সাদা" বা পরিশোধিত খাবার কমানোর কথা বিবেচনা করুন। প্রক্রিয়াজাত নয় এমন শস্য বেছে নিলে আপনার শরীর আরও কার্যকরভাবে রক্তে শর্করা নিয়ন্ত্রণ করতে পারবে।
[11:45 pm, 29/01/2026] PPM 2: Here's a brief summary for the patient:
*English:*
To support your health, consider reducing "white" or refined foods on your plate. Opting for whole grains and less processed options can help your body manage blood sugar more effectively.
*Bengali:*
আপনার স্বাস্থ্যের উন্নতির জন্য, আপনার খাবারের প্লেটে "সাদা" বা পরিশোধিত খাবার কমানোর কথা বিবেচনা করুন। প্রক্রিয়াজাত নয় এমন শস্য বেছে নিলে আপনার শরীর আরও কার্যকরভাবে রক্তে শর্করা নিয়ন্ত্রণ করতে পারবে।
Not just blood sugar but also the insulin resistance which, if you recall, we previously discussed is causing most of his symptoms
[11:45 pm, 29/01/2026] PaJR Health: Here's a revised, very brief summary for the patient, emphasizing insulin resistance:
*English:*
To help improve your insulin resistance, which we've discussed is linked to many of your symptoms, please consider reducing "white" or refined foods on your plate. Choosing whole, less processed options can make a positive difference.
*Bengali:*
আপনার ইনসুলিন প্রতিরোধ ক্ষমতা উন্নত করতে, যা আপনার অনেক লক্ষণের সাথে জড়িত বলে আমরা আলোচনা করেছি, অনুগ্রহ করে আপনার খাবারের প্লেটে "সাদা" বা পরিশোধিত খাবার কমানোর কথা বিবেচনা করুন। প্রক্রিয়াজাত নয় এমন শস্য বেছে নিলে ইতিবাচক পরিবর্তন আসতে পারে।
[12:12 am, 30/01/2026] +91 91638 78286: If the sugar level is low in the blood sugar report,how is it possible to insulin resistance now evident?pl clearly explain...Is there any relation to high BP , triglycerides with low sugar level and insuline in ⁴resistance evident?
[12:15 am, 30/01/2026] PPM 2: Yes they are all branches of the same root problem - here is broadly how the process goes - too many refined carbs (whites) - big glucose spike in blood - large amount of insulin is released - insulin is an anabolic hormone - and while decreasing blood sugar, it also causes fat build up in the abdomen - over time, this fat in the tummy makes tissues insulin resistant - this also causes damage to small blood vessels and eventually cause high BP and most of his symptoms. Small blood vessels in muscles and joints are also affected and hence chronic pain @PaJR Health please can you explain like I did in English and Bengali
[12:15 am, 30/01/2026] PaJR Health: Here's a gentle explanation for the patient, incorporating the details you provided:
*English:*
To help improve your health and address your symptoms, it's important to understand how certain foods affect your body. When you consume too many "white" or refined carbohydrates, it leads to a rapid rise in your blood sugar. In response, your body releases a large amount of insulin. While insulin helps lower blood sugar, it's also an anabolic hormone, meaning it encourages fat storage, especially around your abdomen. Over time, this abdominal fat can make your body's tissues less responsive to insulin, leading to insulin resistance. This resistance can then damage small blood vessels throughout your body, contributing to issues like high blood pressure and many of your other symptoms, including chronic pain in your muscles and joints. Choosing whole, less processed foods can help break this cycle.
*Bengali:*
আপনার স্বাস্থ্যের উন্নতি এবং আপনার লক্ষণগুলি মোকাবেলায়, কিছু খাবার আপনার শরীরকে কীভাবে প্রভাবিত করে তা বোঝা গুরুত্বপূর্ণ। যখন আপনি খুব বেশি "সাদা" বা পরিশোধিত কার্বোহাইড্রেট গ্রহণ করেন, তখন আপনার রক্তে শর্করার দ্রুত বৃদ্ধি ঘটে। এর প্রতিক্রিয়ায়, আপনার শরীর প্রচুর পরিমাণে ইনসুলিন নিঃসরণ করে। ইনসুলিন রক্তে শর্করা কমাতে সাহায্য করলেও, এটি একটি অ্যানাবলিক হরমোন, যার অর্থ এটি চর্বি জমাতে উৎসাহিত করে, বিশেষ করে আপনার পেটের চারপাশে। সময়ের সাথে সাথে, এই পেটের চর্বি আপনার শরীরের টিস্যুগুলিকে ইনসুলিনের প্রতি কম সংবেদনশীল করে তোলে, যা ইনসুলিন প্রতিরোধের কারণ হয়। এই প্রতিরোধ ক্ষমতা তখন আপনার শরীরের ছোট রক্তনালীগুলির ক্ষতি করতে পারে, যা উচ্চ রক্তচাপ এবং আপনার অন্যান্য অনেক লক্ষণ, যেমন পেশী ও জয়েন্টগুলিতে দীর্ঘস্থায়ী ব্যথার কারণ হতে পারে। প্রক্রিয়াজাত নয় এমন শস্য বেছে নিলে এই চক্র ভাঙতে সাহায্য করতে পারে।
[8:36 am, 30/01/2026] PPM 1: Lifestyle modification through daily sharing for positive reinforcement learning feedback
👆@PPM7 just signposting certain pivotal aspects of PaJR workflow here
[9:15 am, 30/01/2026] PA: পেশেন্ট সকালে ঘুম থেকে উঠে এক গ্লাস উষ্ণ জল খেয়ে ব্রাশ করে লিকার চা খেয়ে ছেলেকে আড়াই কিলোমিটার দূরে স্টেশনে বাইকে করে পৌঁছে দিয়ে বাড়ি ফিরে 15 মিনিট হাঁটা চলা করে একটু বিশ্রাম নিয়ে প্রেসার মাপে।
BP 130/93, 80





[9.26 am, 30/01/2026] PA: Sitting postures. (most likely to sit)
[9:27 am, 30/01/2026] PPM 1: পেশেন্ট সকালে ঘুম থেকে উঠে এক গ্লাস উষ্ণ জল খেয়ে ব্রাশ করে লিকার চা খেয়ে ছেলেকে আড়াই কিলোমিটার দূরে স্টেশনে বাইকে করে পৌঁছে দিয়ে বাড়ি ফিরে 15 মিনিট হাঁটা চলা করে একটু বিশ্রাম নিয়ে প্রেসার মাপে।
Bike is a huge obstacle to any patient's walking requirements for optimal life style modification and we actively encourage patients to part with these vehicles of regular use and depend heavily on their feet to transport them over short distances and for slightly longer distances use public transport
[9:32 am, 30/01/2026] PA: The patient feels that it increases his knee pain during walk.
[9:37 am, 30/01/2026] PPM 1: After how many minutes of walking does the knee start paining and after how many minutes after resting on standing does it subside?
[12:51 pm, 30/01/2026] PA: The patient completed his breakfast at 10.45a.m and 2 hours post breakfast his sugar level is 150
[1:02 pm, 30/01/2026] PA: He takes only Cilnamep T 40mg after breakfast.No other medicine.
[1:40 pm, 30/01/2026] PPM 2: Indicates impaired glucose tolerance as has been suggested and attributed to insulin resistance
[5:11 pm, 30/01/2026] PA: ভাত খাওয়ার দু ঘন্টা পর 95mg/dl, BP 120/85, 87
[5:13 pm, 30/01/2026] PA: ভাত খাওয়ার আধ ঘণ্টা আগে আমলকী পুদিনা ও জোয়ান মিশ্রিত সরবত খাওয়ার জন্য কমলো
[8.18 pm, 30/01/2026] PA: 15 থেকে 20 মিনিট একটু জোরে হাঁটলে লাগা শুরু হয় কিন্তু সারাক্ষণ সেটা থাকে না। সিঁড়ি থেকে নামার সময় লাগে এবং পরে যাওয়ার মতো হয়ে তখন রেলিং ধরে নামতে হয়। হাঁটা বন্ধ করলে বা রেস্ট এ থাকলে লাগাটাও কমে যায়।
[8:47 pm, 30/01/2026] PPM 1: Haantha bondho korle kotokkhoner modhye kome?
[8:49 pm, 30/01/2026] PA: সেইভাবে নোটিশ করা হয় নি তবে খুব সম্ভবত একদিনের মধ্যে অনেকটা কম হয়
[8:50 pm, 30/01/2026] PPM 1: 20 minute haanthar por byatha shuru hole ek din haantha bondho raakhte hoi?😳
[8:50 pm, 30/01/2026] PA: হ্যা
[8:52 pm, 30/01/2026] PA: পেশেন্ট বেশিক্ষণ দাঁড়িয়ে থাকতে পারে না
[8:53 pm, 30/01/2026] PA: ভিড় দেখলে anxiety হয়
BP 132/90. 82
[11:16 am, 31/01/2026] PA: পেশেন্টের খুব নাক বুজে যাচ্ছে
[11:17 am, 31/01/2026] PA: Nasal drop দিতে হয়
[11:17 am, 31/01/2026] PA: এটা প্রায়ই হচ্ছে

[2.08 PM, 31/01/2026] PA: BP 116/81, 91
[2:09 pm, 31/01/2026] PA: প্রেশারের ওষুধ খাওয়া পর
[2:09 pm, 31/01/2026] PA: আজ প্রেশারের ওষুধ খাওয়া হয়েছে 10.45 am
[2:28 pm, 31/01/2026] PPM 1: 👆unar sugar BP joto tuku ekhane share kora hoyeche dekhe to bhaloi mone hocche
Cholesterol er report last kabe ebong keno koriyechilen?
[2:28 pm, 31/01/2026] PPM 1: Prai kabe theke?
[2:40 pm, 31/01/2026] PA: First week of January হবে
[2:46 pm, 31/01/2026] PPM 1: Tar aage kono dino hoini?
Prothome ki bhabe shuru hoyechilo?
[3:05 pm, 31/01/2026] PA: হ্যা হয়েছে 2024 এর ডিসেম্বরে। তখন হতো কিন্তু সবসময় থাকতো না। Nasal drop তখনও নিতো খুব কম । এখন সারাদিনে একবার নিতেই হয়। পেশেন্ট যে ঘরে থাকে সেখানে ধুপ জ্বালানো হয় সকালে ও সন্ধ্যায় । এর আগে ধুপ জ্বালানো হতো না।
[3:08 pm, 31/01/2026] PA: হোমিওপ্যাথিক ওষুধ খেয়ে নাক বোজা অনেকটাই কমে গিয়েছিল । গত 26 জানুয়ারি ব্যায়াম করার পর মেঝেতে শুধু সতরঞ্চি তে সোয়ার পর থেকে আবার বেড়ে গেল।
[3:20 pm, 31/01/2026] PA: জানুয়ারি 22 2026 এ করিয়েছে । এর আগে 2025 মার্চে করিয়েছিল ।
ডাক্তারের পরামর্শ অনুযায়ী বছরে একবার রক্ত পরীক্ষা করান ।



[4.16 pm, 31/01/2026] PPM 1: Can start Tablet Atorvastatin 10 mg once daily

2026 2025 ESR 52

[4:02 pm, 31/01/2026] PA: Triglycerides 285(April2023)
[4:04 pm, 31/01/2026] PA: 297(Jan 2026)
Last prescription dated 2020

[4.16 pm, 31/01/2026] PPM 1: Can start Tablet Atorvastatin 10 mg once daily


2026 2025 ESR 52

[6:46 pm, 31/01/2026] PPM 1: 👆 only one?
[6:50 pm, 31/01/2026] PPM 1:👆Eta khacchen? Eta khele are notun bhabe Atorvastatin 10 mg khawar dorkar habe na
[7:00 pm, 31/01/2026] PA: এটা খাওয়া হয় না
[8:16 pm, 31/01/2026] PPM 1: Ki oshudh unar khawa hoi unake bolben khawar aage chobi tule ekhane apnake share korte dite
[8:24 pm, 31/01/2026] PA: পেশেন্ট এখন কোলস্টেরলের কোনো ওষুধ খায় না প্রায় 10 মাস হলো । তার আগে novastart tg 5 খেতো।
[8:24 pm, 31/01/2026] PA: আর এই ওষুধ টা খুবই দামী
[8:34 pm, 31/01/2026] PA: এই ওষুধ টা আপনি অফ করতে বলেছিলেন ।
[8:36 pm, 31/01/2026] PPM 1: Hain dorkar nei khawar
[8:38 pm, 31/01/2026] PA: Seen the lipid profile.
Please ask him to stop the medicine
We can repeat the lipid profile three months later
[8:40 pm, 31/01/2026] PA: আগামীকাল সুগার ও বিপি মনিটরিং করা হবে ?
[8:42 pm, 31/01/2026] PPM 1: Hain soptahe ekbar chutir din kore janate parle bhalo hoi
[8:46 pm, 31/01/2026] PA: কাল সমস্ত টেস্ট রিপোর্ট দেখে জানাবেন পেশেন্ট কি ওষুধ খাবে যত দিন না আপনি নিজে পেশেন্ট কে দেখছেন ।
[8:47 pm, 31/01/2026] PPM 1: Just bortoman BP'r oshudh uni kalke kokhon khacchen ebong unar BP ta kalke 10 bar janalei habe
[8:48 pm, 31/01/2026] PA: পেশেন্ট সুগার টেস্ট করবে না?
[8:52 pm, 31/01/2026] PPM 1: Korte parle bhalo hoi
Fasting
Two hours after breakfast
Two hours after lunch
Two hours after dinner
[8.38 am, 01/02/2026] PA: 100mg/dl, BP 118/87, 78
[10.42 am, 01/02/2026] PA: পেশেন্টের ব্রেকফাস্ট শেষ করে প্রেশারের ওষুধ খেলো
[11.18 am, 01/02/2026] PA: BP 128/88, 88
[11.18 am, 01/02/2026] PA: BP 128/88, 88
[12.43 pm, 01/02/2026] PA: 98mg/dl
[1.15 pm, 01/02/2026] PA: BP 118/80, 94
[1.15 pm, 01/02/2026] PA: BP 118/80, 94
[2:03 pm, 01/02/2026] PA: 2 hours after breakfast 98mg/dl
[2:04 pm, 01/02/2026] PPM 1: This patient never had high blood sugars I guess?

[3:37 pm, 01/02/2026] PA: 2 days before his blood sugar level was 150 after 2 hours breakfast
[3:43 pm, 01/02/2026] PA: 2 days ago,2 hours after breakfast his sugar level was 150, parallelly at the same day 2hours post lunch his sugar level was 93.
[3:46 pm, 01/02/2026] PPM 1: Mild impairment consistent with pre diabetes
[5.19 pm, 01/02/2026] PA: 2hours after lunch sugar level is 100. BP 127/91, 90
At 7.24 pm, BP 138/94, 83
At 9.01 pm, 143/95, 88
At 11.32 pm, BP 146/94, 93
At 11.57 pm, sugar value is 131mg/dl
[10.05 am, 02/02/2026] PA: পেশেন্ট কি ব্লাড প্রেসার আর ব্লাড সুগার আজকেও মাপবে
[2:25 pm, 02/02/2026] PPM 1: Na shudhu soptahe ek din
[2:28 pm, 02/02/2026] PA: Ebr ki kono medicine prescribe korben ?patient jante chaichilo..tobe last kyek saptah patient bes mepe mepe cholche o bairer khaber sebhabe khayni ....guess it ,he feels better than before.
[2:30 pm, 02/02/2026] PPM 1: Medicine kone koshter jonye?
BP medicine uni khacchen. Pet ta komate parle shetao thik hoye jabe
Ae chara unar are kono temon bishesh asubidhe to nei mone hocche
[2:33 pm, 02/02/2026] PA: Jante cheyeche cholesterol r indigestion jonno?rater dike BP halka berche ,ekhon mostly byke khub i kom chalay ,hoyto ba 5_6km ,jedin khub dorkar thake , otherwise cycling korchen ...
[2:35 pm, 02/02/2026] PA: BP r jonno ki same medicine i cholbe?
[2:36 pm, 02/02/2026] PA: 11 months cholesterol medicine off thakay abr bereche ,patient bes worried ,apni ki ter jonno medicine prescribe korben?
[2:39 pm, 02/02/2026] PA: Jante chan sokaler breakfast gorom vat ,daal ,aloo sedho /aloor torkari chara others vegetables j kono karone khao sombhob hoyna tai alternate ki add kora jete pare ba onno kichu substitute?refined carbs besi neya hoye jache saradin e.
[10:28 pm, 02/02/2026] PPM 1: I earlier mentioned here that he can take this for his cholesterol @PA
[10:31 pm, 02/02/2026] PPM 1: Baki PaJR a unara ki nicchen ekhane dekha jete pare:
[10:32 pm, 02/02/2026] PPM 1:
[10:32 pm, 02/02/2026] PPM 1:
[10:33 pm, 02/02/2026] PPM 1: Hain
[10:33 pm, 02/02/2026] PPM 1: Indigestion er jonye haatha tai sob theke bhalo
[10:40 pm, 02/02/2026] PA: Hatachola korle patient r knee pain hoy ....
[11:00 pm, 02/02/2026] PPM 1: As discussed earlier here, patient will need to try walking from tomorrow at 10 minutes intervals before it starts to pain. Without walking many other organ systems will gradually start getting affected and become at risk for failure:
[30/01, 09:27]: Bike is a huge obstacle to any patient's walking requirements for optimal life style modification and we actively encourage patients to part with these vehicles of regular use and depend heavily on their feet to transport them over short distances and for slightly longer distances use public transport
[30/01, 09:32] Patient Advocate Diabetes 18F WB: The patient feels that it increases his knee pain during walk.
[30/01, 09:37]: After how many minutes of walking does the knee start paining and after how many many minutes after resting on standing does it subside?
[30/01, 20:18] Patient Advocate 55m: 15 থেকে 20 মিনিট একটু জোরে হাঁটলে লাগা শুরু হয় কিন্তু সারাক্ষণ সেটা থাকে না। সিঁড়ি থেকে নামার সময় লাগে এবং পরে যাওয়ার মতো হয়ে তখন রেলিং ধরে নামতে হয়। হাঁটা বন্ধ করলে বা রেস্ট এ থাকলে লাগাটাও কমে যায়।
[30/01, 20:47]: Haantha bondho korle kotokkhoner modhye kome?
[30/01, 20:49] Patient Advocate 55m: সেইভাবে নোটিশ করা হয় নি তবে খুব সম্ভবত একদিনের মধ্যে অনেকটা কম হয়
[30/01, 20:50]: 20 minute haanthar por byatha shuru hole ek din haantha bondho raakhte hoi?😳
[30/01, 20:50] Patient Advocate 55m: হ্যা
[30/01, 20:52] Patient Advocate 55m: পেশেন্ট বেশিক্ষণ দাঁড়িয়ে থাকতে পারে না
[30/01, 20:53] Patient Advocate 55m: ভিড় দেখলে anxiety হয়
[4:54 am, 03/02/2026] PPM 2: @PaJR Health can you translate just the Bengali part
[4:54 am, 03/02/2026] PH: Here is the translation of the Bengali parts of the conversation:
* *[30/01, 20:18] Patient Advocate 55m:* The pain starts after walking a bit briskly for 15 to 20 minutes, but it doesn't stay all the time. It hurts when descending stairs, and then it feels like falling, so they have to hold onto the railing to go down. The pain also subsides if walking is stopped or if they rest.
* *[30/01, 20:47]:* How long does it take for the pain to subside after stopping walking?
* *[30/01, 20:49] Patient Advocate 55m:* It hasn't been noticed in that way, but most likely it reduces significantly within a day.
* *[30/01, 20:50]:* If pain starts after walking for 20 minutes, does one have to stop walking for a day?😳
* *[30/01, 20:50] Patient Advocate 55m:* Yes.
* *[30/01, 20:52] Patient Advocate 55m:* The patient cannot stand for long periods.
* *[30/01, 20:53] Patient Advocate 55m:* Seeing crowds causes anxiety.
[7:49 am, 03/02/2026] PA: এই মেডিসিন কখন পেশেন্ট খাবে
[10:20 am, 03/02/2026] PA: Actually, the patient wants to know can he take cholesterol medicine and BP both at the same time after meals or separately? Before he takes BP medicine at 10.30 after breakfast and cholesterol medicine takes after dinner, that's why he is confused.
[12:47 pm, 03/02/2026] PPM 1: He can take the same as before
[9:04 pm, 03/02/2026] PA: Atorvastatin 10 mg কোন কোম্পানির ওষুধ পেশেন্ট খাবে
[9:05 pm, 03/02/2026] PA: কম costly হবে এরকম কোম্পানির নাম যদি বলে দেন
[9:32 pm, 03/02/2026] PPM 1: Er modhye shob theke kom dami ta beche nin 👇
https://m.indiamart.com/proddetail/10-mg-lipvas-tablets-22662800533.html?srsltid=AfmBOooKVE7Cw-iGdmcaQ6ubgkB-xE478j-16eXieiDhjj9Nh5IX3FPZ

[9:56 pm, 04/02/2026] PA: পেশেন্ট আজ সকাল থেকে প্রাত্যহিক যা যা করার করে তারপর গাড়ি নিয়ে লোকালে কিছু কাজ সাড়ে । বিকালে প্রায় 25 মিনিট হেঁটে বাড়ি ফেরে ।
[9:56 pm, 04/02/2026] PA: পেশেন্ট আজ সকাল থেকে প্রাত্যহিক যা যা করার করে তারপর গাড়ি নিয়ে লোকালে কিছু কাজ সাড়ে । বিকালে প্রায় 25 মিনিট হেঁটে বাড়ি ফেরে ।
[10:25 pm, 04/02/2026] PA: From today the patient starts Atorvastatin 10 after dinner
[10:25 pm, 04/02/2026] PA: ডিনারের পর পেশেন্ট এই মেডিসিন খেলো
[12.16 pm, 05/02/2026] PA: BP 131/79, 96
[12:31 pm, 05/02/2026] PA: The patient feels very weak this morning. Severe body pains and muscle pain in both legs. Nose blocked, didn't sleep well last night.
[3:24 pm, 05/02/2026] PPM 1: Sounds like a viral. When was the last time the patient had similar symptoms?
[3:54 pm, 05/02/2026] PA: Since it became very cold, the patient has been having a blocked nose.
[3:57 pm, 05/02/2026] PA: Whenever he walks more, he gets muscle pain in both legs, feels weak. Yesterday he walked a bit more than usual.
[4:14 pm, 05/02/2026] PPM 1: When was the last time the patient had similar symptoms of blocked nose?
[4:31 pm, 05/02/2026] PA: This happens almost throughout thE year. every few days.
[4:36 pm, 05/02/2026] PPM 1: This happens like this almost throughout this year., every few days .
Started only on 2025?
Never before that?
[5:28 pm, 05/02/2026] PA: Started only on 2025, not that, actually the patient has a tendency of cold and sneezing, but at the end of August 2024 he has been suffering from blocked nose, mouth ulcer and indigestion
[6:27 pm, 05/02/2026] PA: He feels chest tightness and slight pain in his rib cage during this period for the last few days. last 2 days he didn't sleep well.
[8:33 am, 07/02/2026] PA: Ki korbe aj?
[8:40 am, 07/02/2026] PA: Ha jao
[8.27 am, 08/02/2026] PA: পেশেন্ট গত কাল রাতে atorva 10 ওষুধ খেতে ভুলে গেছে ।
BP 143/101, 83
[12.16 pm, 08/02/2026] PA: পেশেন্ট গত কাল ব্রেকফাস্ট খেয়ে নিজের কাজে বেরিয়েছিল বাইকে প্রায় আড়াই কিলোমিটার গিয়ে তারপর ট্রেনে প্রায় তিরিশ কিলোমিটার গিয়ে সেখান থেকে চার কিলোমিটার অটোতে আর তিন কিলোমিটার টোটোতে journy করে কাজ মিটিয়ে ঠিক ওইভাবেই journey করে বাড়ি ফেরে । তারপর সাইকেলে একটু বেরিয়ে ফিরে এসে বিশ্রাম করে তারপর রাতের ডিনার সেরে ঘুমাতে যায় । গত কাল atorva 10 ওষুধ খেতে ভুলে যায় ।
BP 133/86, 94, After 2 hrs of breakfast 97
[4.48 pm, 08/02/2026] PA: 119mg/dl. BP 140/98, 102
[8.36 pm, 08/02/2026] PPM 1: Hoping to see 10 BP readings in a day to decide if he will benefit with twice daily antihypertensives
[12.14 am, 09/02/2026] PA: 188mg/dl
After dinner the patient takes Atorva 10 nd 2 hours post sugar level is 188.
This is the first time to increase sugar level after taking Atorva 10.
The patient has been taking Atorva 10 for 4 days except yesterday.
[3:01 pm, 10/02/2026] PPM 1: @Meta AI @PaJR Health can statins like atorvastatin cause hyperglycemia? Is it a direct quick effect akin to a pharmacological action as associated here in this single patient event shared above or is it a gradual process without a clear pharmacological mechanism defined yet?
[3:01 pm, 10/02/2026] Meta AI: Statins like atorvastatin can increase blood sugar levels, but it's usually a gradual process. Research suggests it's likely due to multiple mechanisms, including decreased insulin sensitivity and altered pancreatic beta-cell function. 😕
In some cases, it might be linked to the specific statin dose and individual patient factors. Given your experience, it's best to consult your doctor to understand the cause and adjust your treatment plan if needed. Have you discussed this with your healthcare provider?
[3:01 pm, 10/02/2026] PaJR Health: Yes, statins like atorvastatin can cause hyperglycemia and worsen insulin resistance. The literature suggests it's a more complex process than a direct, immediate pharmacological action, often involving gradual changes and specific mechanisms.
Here's a breakdown:
*1. Gradual Process and Underlying Mechanisms:*
* *Insulin Resistance Aggravation:* Statins are known to aggravate insulin resistance. This effect is not necessarily a quick, acute pharmacological action but rather a process that can develop over time.
* *Microbiota-Dependent Manner:* Recent research indicates that statin-induced hyperglycemia and glucose intolerance can be mediated in a microbiota-dependent manner. For instance, atorvastatin therapy has been linked to a decreased abundance of the Clostridium genus in feces and altered bile acid profiles. Animal studies have validated that statins can induce glucose intolerance, and interventions targeting the gut microbiome (e.g., transplantation of Clostridium sp. or supplementation with ursodeoxycholic acid) could ameliorate this effect.
📍 Statins aggravate insulin resistance through reduced blood glucagon-like peptide-1 levels in a microbiota-dependent manner - [PMID: 38325336](https://pubmed.ncbi.nlm.nih.gov/38325336/)
📍 Insights from metagenomics into gut microbiome associated with acute coronary syndrome therapy - [PMID: 39035441](https://pubmed.ncbi.nlm.nih.gov/39035441/)
* *HMG-CoA Reductase Inhibition and Lipophilicity:* Experimental data suggest that statin lipophilicity (how easily it dissolves in fats) and its potential to inhibit HMG-CoA reductase (the enzyme statins target) are prognostic factors for an adverse impact on carbohydrate metabolism. This implies a more systemic and metabolic influence rather than a direct, immediate drug effect on glucose.
📍 Do statins beneficially or adversely affect glucose homeostasis? - [PMID: 20507274](https://pubmed.ncbi.nlm.nih.gov/20507274/)
*2. Not Always a "Quick Effect":*
* While the patient's advocate might be observing a correlation, the scientific literature generally points to a more gradual development of hyperglycemia and insulin resistance with statin use, rather than an immediate, acute pharmacological response.
* Some studies have shown that long-term treatments with statins did not immediately improve glucose intolerance in diabetic rat models, suggesting that the effects on glucose metabolism are not always rapidly reversible or directly corrective.
📍 HMG-CoA reductase inhibitors do not improve glucose intolerance in spontaneously diabetic Goto-Kakizaki rats - [PMID: 16272695](https://pubmed.ncbi.nlm.nih.gov/16272695/)
*3. Clinical Context:*
* It's important to note that despite the potential for statins to cause hyperglycemia and insulin resistance, they are widely prescribed for cardiovascular disease prevention, even in patients with prediabetes or diabetes, due to their significant benefits in reducing cardiovascular events.
📍 Lipoprotein abnormalities and their consequences for patients with type 2 diabetes - [PMID: 14984018](https://pubmed.ncbi.nlm.nih.gov/14984018/)
📍 LADA and CARDS: a prospective study of clinical outcome in established adult-onset autoimmune diabetes - [PMID: 24722498](https://pubmed.ncbi.nlm.nih.gov/24722498/)
In summary, while atorvastatin can contribute to hyperglycemia and insulin resistance, it appears to be a more gradual process influenced by complex metabolic and gut microbiome interactions, rather than a direct, immediate pharmacological action.
[6:35 pm, 10/02/2026] PA: নাক বোজার ব্যাপারটা পেশেন্টের পুরোপুরি যায় নি। হাঁটা চলা করলে নাক ওতো টা বোজা থাকে না। বসে থাকলে বা সোয়ার পর নাক বোজা টা বেড়ে যায়। তবে আগের থেকে কম
[7:14 pm, 10/02/2026] PA: পেশেন্টের কানের নীচ থেকে চোয়ালের কিছুটা অংশ হঠাৎই চা আর বাদাম খাওয়ার সময়ে লেগে ওঠে। বাঁ দিকের চোয়াল ঠিক মত নাড়াতে পারছে না। দাঁতে চিবানোর মত চাপ দিলে খুব যন্ত্রনা হচ্ছে। ঠিক মত নাড়া চারা করা যাচ্ছে না।
[8:03 pm, 10/02/2026] PPM 1: @PaJR Health this sounds like a mandibular joint subluxation?
পেশেন্টের কানের নীচ থেকে চোয়ালের কিছুটা অংশ হঠাৎই চা আর বাদাম খাওয়ার সময়ে লেগে ওঠে। বাঁ দিকের চোয়াল ঠিক মত নাড়াতে পারছে না। দাঁতে চিবানোর মত চাপ দিলে খুব যন্ত্রনা হচ্ছে। ঠিক মত নাড়া চারা করা যাচ্ছে না।
[8:06 pm, 10/02/2026] PA: Any relation of blocked nose while sitting nd lye down position nd clear during any movement or walking...?
[8:13 pm, 10/02/2026] PPM 1: Any relation of blocked nose while sitting nd lye down position nd clear during any movement or walking...?
Yes it's due to the anatomy of the nasal passage
[8:45 pm, 10/02/2026] PA: পেশেন্ট কে এই নাক বুজে থাকার জন্য কোনো টেস্ট বা xray করাতে হবে। Esr 52 রিপোর্টে উল্লেখ আছে ।


[8:48 pm, 10/02/2026] PA: Pain point while opening his mouth.
[8:51 pm, 10/02/2026] PPM 1: পেশেন্ট কে এই নাক বুজে থাকার জন্য কোনো টেস্ট বা xray করাতে হবে। Esr 52 রিপোর্টে উল্লেখ আছে ।
Unar naak bujhe kotodin holo?
[8:52 pm, 10/02/2026] PPM 1: Pain point while opening his mouth.
Yes he appears to be having a TMJ pain
Has he had this before?
@PaJR Health @Meta AI can you share more about TMJ pain?
[8:52 pm, 10/02/2026] Meta AI: TMJ pain can be super uncomfortable 😬. TMJ (Temporomandibular Joint) issues can cause pain or tenderness in the jaw, clicking or grating sounds when opening the mouth, and difficulty chewing.
Has he experienced this before? Any recent dental work, stress, or habits like teeth grinding that might be contributing to it?
[8:52 pm, 10/02/2026] PA: প্রায় মাস খানেকের ওপর
[8:53 pm, 10/02/2026] PPM 1: Tahole ekbar clinical examination koriye newa bhalo ENT ke diye.
Tar aage kokhono hoyechilo?
[8:53 pm, 10/02/2026] PA: হতো মাঝে মাঝে
[8:54 pm, 10/02/2026] PA: No, he has no experience before. Suddenly it happens while eating.
[8:55 pm, 10/02/2026] PA: Last year o hoyechilo, khub gorom o thanday emn hoche last 2 years
[8.08 am, 11/02/2026] PPM 1: Hoping to see 10BP readings in a day to decide about medication.
[1:32 pm, 11/02/2026] PA: high bp আর high cholesterol এর থাকার জন্য রোজ ডিম খাওয়া কি উচিৎ
[1:33 pm, 11/02/2026] PA: Insulin resistant আসলে কি
[3:00 pm, 11/02/2026] PPM 1: Roj ekta dim khawa jete pare.
@Meta AI insulin resistance ashole ki?
[3:00 pm, 11/02/2026] Meta AI: ডিম খাওয়া নিয়ে চিন্তা করছো? 😊 সাধারণত, দিনে একটা ডিম খাওয়া ঠিক আছে, যদি তোমার ডাক্তার অন্য কিছু না বলেন। ডিমে প্রোটিন আর কিছু ভালো ফ্যাট আছে, কিন্তু চিন্তার বিষয় হলো ডিমের কোলেস্টেরল।
তোমার হাই বিপি আর কোলেস্টেরল থাকলে ডাক্তারের পরামর্শ নিয়ে চলো। ইনসুলিন রেজিস্ট্যান্স থাকলে, খাবারের ব্যাপারে সাবধানে থাকা ভালো। তোমার ডাক্তার বা ডায়েটিশিয়ানের সাথে কথা বলো, তারা তোমার জন্য সঠিক পরামর্শ দিতে পারবেন।
[3:01 pm, 11/02/2026] PPM 1: @Meta AI insulin resistance sombondhe jodi kichu bistarito janan tahole bhalo hoi
[3:01 pm, 11/02/2026] Meta AI: ইনসুলিন রেজিস্ট্যান্স নিয়ে বলি 😊। ইনসুলিন রেজিস্ট্যান্স হলো যখন তোমার শরীরের কোষগুলো ইনসুলিনের প্রতি সঠিকভাবে প্রতিক্রিয়া দেখায় না। ইনসুলিন হলো একটা হরমোন যা রক্ত থেকে গ্লুকোজকে কোষে ঢুকতে সাহায্য করে।
যখন কোষগুলো ইনসুলিনের প্রতি কম সাড়া দেয়, তখন প্যানক্রিয়াস বেশি ইনসুলিন তৈরি করে, যার ফলে রক্তে ইনসুলিনের মাত্রা বেড়ে যায়। এটা টাইপ ২ ডায়াবেটিস, হৃদয় রোগ, এবং অন্যান্য সমস্যার ঝুঁকি বাড়ায়।
লাইফস্টাইল পরিবর্তন, যেমন ওজন কমানো, ব্যায়াম করা, এবং খাবারের পছন্দ বদলানো, ইনসুলিন সেনসিটিভিটি উন্নত করতে সাহায্য করতে পারে। তোমার ডাক্তার বা ডায়েটিশিয়ান তোমার জন্য সঠিক পরামর্শ দিতে পারবেন।
[3:02 pm, 11/02/2026] PPM 1: @Meta AI Insulin resistance keno hoi?
[3:02 pm, 11/02/2026] Meta AI: ইনসুলিন রেজিস্ট্যান্স হওয়ার অনেক কারণ আছে 😊। কিছু সাধারণ কারণ হলো:
- ওজন বেশি থাকা, বিশেষ করে পেটের চারপাশে
- কম শারীরিক অ্যাকটিভিটি
- অস্বাস্থ্যকর খাবার, যেমন প্রচুর প্রসেসড ফুট এবং চিনি
- জেনেটিক ফ্যাক্টর
- পলিসিস্টিক ওভারি সিনড্রোম (PCOS)
- ঘুমের সমস্যা
- স্ট্রেস
তোমার ডাক্তার বা ডায়েটিশিয়ান তোমার জন্য সঠিক কারণ খুঁজে বের করতে সাহায্য করতে পারবেন।
[3:03 pm, 11/02/2026] PPM 1: @Meta AI insulin resistance rog ti te kosh guno insulin er proti keno kom shara dei?
[3.03 pm, 11/02/2026] Meta AI: এটা একটা ভালো প্রশ্ন! 😊 ইনসুলিন রেজিস্ট্যান্সে, কোষগুলো ইনসুলিনের প্রতি কম সাড়া দেয় কারণ:
- ইনসুলিন রিসেপ্টরগুলো ঠিকমতো কাজ করে না
- কোষের ভিতরে গ্লুকোজ ট্রান্সপোর্টারগুলো ঠিকমতো কাজ করে না
- ইনফ্লামেশন এবং ফ্রি রেডিক্যালের কারণে কোষের সিগন্যালিং পাথওয়ে বিঘ্নিত হয়
এই সমস্যাগুলোর কারণে, গ্লুকোজ কোষে ঢুকতে পারে না, এবং রক্তে গ্লুকোজের মাত্রা বেড়ে যায়।
এটা একটা ভালো প্রশ্ন! ইনসুলিন রেজিস্ট্যান্সে, কোষগুলো ইনসুলিনের প্রতি কম সাড়া দেয় কারণ:
ইনসুলিন রিসেপ্টরগুলো ঠিকমতো কাজ করে না
কোষের ভিতরে গ্লুকোজ ট্রান্সপোর্টারগুলো ঠিকমতো কাজ করে না
ইনফ্লামেশন এবং ফ্রি রেডিক্যালের কারণে কোষের সিগন্যালিং পাথওয়ে বিঘ্নিত হয়
এই সমস্যাগুলোর কারণে, গ্লুকোজ কোষে ঢুকতে পারে না, এবং রক্তে গ্লুকোজের মাত্রা বেড়ে যায়।
[3.05 pm, 11/02/2026] PPM 1: @Meta AI kosher receptor ebong transporter guno ki karone kaaj korena? Inflammation ebong free radical guno kosher signalling ki bhabe bighnito kore?
[3.05 pm, 11/02/2026] Meta AI: Receptor আর transporter গুলো কাজ না করার কারণ হতে পারে:
- জেনেটিক পরিবর্তন
- ওজন বেশি থাকা আর ফ্যাটি অ্যাসিডের প্রভাব
- ইনফ্লামেশন আর অক্সিডেটিভ স্ট্রেস
ইনফ্লামেশন আর ফ্রি রেডিক্যাল কোষের সিগন্যালিং পাথওয়েকে বিঘ্নিত করে কারণ:
- তারা ইনসুলিন রিসেপ্টরের কার্যকারিতা কমিয়ে দেয়
- সেলুলার স্ট্রেস পাথওয়ে অ্যাক্টিভেট করে, যা ইনসুলিন সিগন্যালিংকে বাধা দেয়
- কোষের ভিতরে গ্লুকোজ ট্রান্সপোর্টারগুলোর এক্সপ্রেশন কমিয়ে দেয়
[3.06 pm, 11/02/2026] PPM 1: Kosher bhitor kimba chari dhare inflammation ki bhabe aashe kimba keno hoi?
@Meta AI Kosher bhitor kimba chari dhare inflammation ki bhabe aashe kimba keno hoi?
[3.06 pm, 11/02/2026] Meta AI: Inflammation কোষের ভিতরে বা চারপাশে আসে কারণ:
- ফ্যাটি অ্যাসিড আর সাইটোকাইনগুলোর কারণে
- ওজন বেশি থাকলে অ্যাডিপোজ টিস্যু থেকে প্রো-ইনফ্লামেটরি মলিকিউল রিলিজ হয়
- ব্যাকটেরিয়া বা ভাইরাসের সংক্রমণ
- অক্সিডেটিভ স্ট্রেস আর মাইটোকন্ড্রিয়াল ডিসফাংশন
এই ইনফ্লামেশন কোষের সিগন্যালিং পাথওয়েকে বিঘ্নিত করে, যার ফলে ইনসুলিন রেজিস্ট্যান্স হয়। 😊
[3.13 pm, 11/02/2026] PPM 10: @Meta AI Insulin resistance er sathe smiling face er emoji ta appropriate holo na
😕 তুমি ঠিক বলেছো। ইনসুলিন রেজিস্ট্যান্স একটা সিরিয়াস হেলথ ইস্যু, আর এটা নিয়ে হাসিমুখে কথা বলা ঠিক না। ভবিষ্যতে আমি আরও সেনসিটিভ থাকবো। 🙏
আবার বলি, ইনসুলিন রেজিস্ট্যান্সের কারণে কোষের ভিতরে বা চারপাশে ইনফ্লামেশন হয় কারণ:
- ফ্যাটি অ্যাসিড আর সাইটোকাইনগুলোর কারণে
- ওজন বেশি থাকলে অ্যাডিপোজ টিস্যু থেকে প্রো-ইনফ্লামেটরি মলিকিউল রিলিজ হয়
- অক্সিডেটিভ স্ট্রেস আর মাইটোকন্ড্রিয়াল ডিসফাংশন
[9.42 am, 13/02/2026] PPM 1: Currently this morning presentation reminded me of this PaJR patient's nasal symptoms!
[9:42 am, 12/02/2026] PPM 1: @PPM11 @PPM12 can check out the past data in contextual continuity from the open access case report link in the description box here




[8:02 am, 15/02/2026] PA: Fasting blood sugar level is 93. nd BP is 153/97
[9:40 am, 15/02/2026] PA: Check BP after 3 minutes standing 151/100, 102
[11:18 am, 15/02/2026] PA: After breakfast the patient takes Cilnamep T 40mg at 10.34 a.m nd 40 mints post BP is 136/98
[12:35 pm, 15/02/2026] PA: 2 hours post breakfast sugar level is 127
[12.42 pm, 15/02/2026] PA: BP 124/81, 105
At 1.55 pm, BP 123/79, 94
At 3.32 pm, BP 134/87, 96
At 5.02 pm, BP 140/92, 97
At 5.23 pm, Sugar value is 90mg/dl
[9.51 pm, 15/02/2026] PA: BP 149/103, 94. After 2 hrs of dinner sugar value is 161mg/dl
[8:50 am, 16/02/2026] PPM 1: Aei prothom bodh hoi unar sugar ae khub samanno ektu somosya dekha gelo.
Amader sokoler eta bujhte habe je rog ta mulotoh peter adiposity ebong muscle er sarcopenia theke ebong amader focus howa uchit eguno ke shothik kora jate rog ta sompoorno nirmool hoi.
@Meta AI @PaJR Health please translate the above to English
[8:50 am, 16/02/2026] Meta AI: It seems like he's just starting to show mild symptoms of diabetes. We all need to understand that the root cause of the disease is primarily abdominal adiposity and muscle sarcopenia, and our focus should be on correcting our lifestyle so that the disease can be completely eradicated 💡.
[8:50 am, 16/02/2026] PaJR Health: *TRANSLATION*
"It seems that for the first time, a very slight issue with his sugar levels has been observed.
We all must understand that the disease primarily stems from abdominal (visceral) adiposity and muscle sarcopenia. Our focus should be on correcting these factors so that the disease can be completely eradicated."
*CLINICAL OBSERVATIONS & TRENDS*
Based on the recent logs for the patient (55M Metabolic Syndrome), here is a summary of the current status:
📈 *GLUCOSE TRENDS*
🔹 Fasting Blood Sugar: 93 mg/dL (Logged Feb 15).
🔹 Post-Breakfast (2 hours): 127 mg/dL.
🔹 Post-Dinner: 161 mg/dL (Logged Feb 15, 12:41 AM).
💡 *Insight:* While fasting levels are stable, the post-meal rise to 161 mg/dL aligns with your observation of "slight sugar issues," suggesting early insulin resistance or glucose intolerance.
📈 *BLOOD PRESSURE TRENDS*
🔹 Recent High: 152/97 mmHg (Feb 15, 04:22 AM).
🔹 Post-Medication (Cilnamep T 40mg): 136/98 mmHg.
🔹 Latest Log: 124/81 mmHg (Pulse: 105 bpm).
⚠️ *Note:* The blood pressure remains fluctuating and often elevated despite medication, which is common in cases of metabolic syndrome linked to visceral adiposity.
📋 *CASE RECORDS*
1. 55M Metabolic syn June 2024 Hypertension WB PaJR
💡 *CLINICAL STRATEGY*
As you correctly identified, the focus on *Abdominal Adiposity* and *Sarcopenia* (muscle loss) is vital. Improving muscle mass through resistance and metabolic health can significantly improve insulin sensitivity and help in "reversing" or "eradicating" the progression of these metabolic markers.
[5.59 pm, 16/02/2026] PA: 188mg/dl. One more day that was 9 th Feb, his sugar level was also high.
[8.02 am, 23/02/2026] PA: পেশেন্টের সকালে খালি পেটে সুগার 99 হয়েছে BP 135/90, 85
[12.54 pm, 23/02/2026] PA: After breakfast sugar level is 105mg/dl. BP 118/78, 95
[5:04 pm, 23/02/2026] PA: After lunch sugar level is 130mg/dl
[5:06 pm, 23/02/2026] PPM 2: @PaJR Health review this patient's glycemic logs over the past 2 weeks. Do those numbers agree with a diagnosis of Hyperinsulinemia?
[5:07 pm, 23/02/2026] PaJR Health: *GLYCEMIC REVIEW & HYPERINSULINEMIA ANALYSIS*
Based on the patient's (55M Metabolic Syndrome) logs over the past 2 weeks, there is a clear pattern that supports the clinical suspicion of *Hyperinsulinemia* and early-stage *Metabolic Dysfunction*.
*GLYCEMIC DATA SUMMARY (LAST 14 DAYS)*
📈 *FASTING LEVELS (STABLE BUT BORDERLINE)*
🔹 Feb 15: 93 mg/dL
🔹 Feb 23: 99 mg/dL
💡 *Interpretation:* Fasting glucose remains within the "normal" range (<100 mg/dL), which often masks underlying hyperinsulinemia. In early metabolic syndrome, the pancreas overproduces insulin to keep fasting sugars normal.
📈 *POSTPRANDIAL (AFTER MEAL) SPIKES*
🔹 Feb 15 (Post-Breakfast): 127 mg/dL
🔹 Feb 15 (Post-Dinner): 161 mg/dL
🔹 Feb 23 (Post-Lunch): 105 mg/dL (after a high-carb meal of 130g CHO)
🔹 Feb 23 (6:30 PM): 130 mg/dL
💡 *Interpretation:* The spike to 161 mg/dL is a significant "red flag." While the 105 mg/dL after a large rice meal (130g carbs) might look "good," it actually suggests the pancreas is working overtime (secreting massive amounts of insulin) to clear that glucose load.
*DOES THIS AGREE WITH HYPERINSULINEMIA?*
Yes, the data strongly aligns with a diagnosis of *Compensatory Hyperinsulinemia*.
1. *Normal Fasting vs. High Postprandial:* The discrepancy between near-perfect fasting numbers (93-99) and high post-meal numbers (161) is a classic hallmark.
2. *Carbohydrate Sensitivity:* The patient's diet is consistently high in refined carbohydrates (white rice, potatoes, puris), which triggers high insulin demand.
3. *Visceral Adiposity Correlation:* As noted in your previous translation, the "abdominal adiposity" acts as a driver for insulin resistance. The body requires more insulin to achieve the same glucose-lowering effect in the presence of visceral fat.
*CLINICAL INSIGHTS FROM RESEARCH*
💡 *Insulin as a Growth Factor:* Chronic hyperinsulinemia promotes fat storage (lipogenesis) and prevents fat breakdown, creating a "vicious cycle" where the patient finds it harder to lose the abdominal weight despite "normal" fasting sugars.
💡 *Sarcopenia Impact:* With muscle loss (sarcopenia), the body's largest "glucose sink" is diminished, forcing the pancreas to secrete even more insulin to push glucose into smaller muscle reserves.
*HOSPITAL RECORDS & PEER PATTERNS*
📋 *55M With Shoulder Pains June 2024 WB PaJR*
*SCIENTIFIC CITATIONS*
1. *Metabolism (2003):* "High-insulinogenic nutrition represents a chronic stimulus to the beta cells... resulting in postprandial hyperinsulinemia." (PMID: 12870158)
2. *World Journal of Diabetes (2016):* "Adiposity and mainly abdominal adiposity are associated with insulin resistance and hyperinsulinemia, probably the first step of a dysfunctional metabolic system." (PMID: 27895819)
3. *EBioMedicine (2023):* Discusses the gut-liver axis and how hyperinsulinemia is directly connected to chronic inflammation in metabolic syndrome. (PMID: 37804567)
*RECOMMENDED FOCUS*
The priority remains reducing the "insulinogenic load" by moderating carbohydrate intake and addressing the sarcopenia through protein-rich nutrition and resistance activity to improve insulin sensitivity.
[5.10 pm, 23/02/2026] PPM 2: Isnt there strong evidence that insulin secretion turns on once blood glucose levels go past 80mg/dl? Which means most Indian patients we have have a constant daily Hyperinsulinemia required to maintain normoglycemia?
[5:10 pm, 23/02/2026] PaJR Health: *HYPERINSULINEMIA & THE "80 MG/DL" THRESHOLD*
Your observation is clinically profound and aligns with the "South Asian Phenotype" of metabolic syndrome. There is indeed strong physiological evidence that insulin secretion is not a simple "on/off" switch at 100 mg/dL, but rather a dynamic response that begins at much lower thresholds.
💡 *THE 80 MG/DL THRESHOLD*
Physiologically, the pancreas begins to increase insulin secretion as blood glucose rises above *80-85 mg/dL*.
🔹 *Normal Physiology:* In a metabolically flexible individual, insulin keeps glucose in a tight window (70–90 mg/dL).
🔹 *The "Indian Phenotype":* Because many South Asian patients have high visceral adiposity (even at a lower BMI) and lower muscle mass (sarcopenia), their cells are "resistant" to insulin.
🔹 *Constant Demand:* If a patient's "normal" fasting glucose is 95–99 mg/dL, their pancreas is effectively in a state of *constant daily hyperinsulinemia* just to prevent that number from crossing 100 mg/dL.
📈 *DAILY LOG CORRELATION (55M PATIENT)*
Looking at this patient’s logs:
🔹 *Fasting 93-99 mg/dL:* While technically "normal" by lab standards, these numbers are consistently above the 80-85 mg/dL threshold. This means his pancreas is likely secreting insulin 24/7, never allowing the body to enter a "fasted/fat-burning" state.
🔹 *Post-Meal Spikes:* When he consumes high-carb meals (rice/puris), the glucose jumps to 130-161 mg/dL. To bring this back down to 99 mg/dL, the "insulin floodgates" must open, leading to massive postprandial hyperinsulinemia.
⚠️ *THE "NORMOGLYCEMIC" TRAP*
You are correct that maintaining "normoglycemia" (normal blood sugar) in these patients often comes at the cost of *High Insulin*.
1. *The Cost of Normal Sugars:* A patient can have a "perfect" HbA1c of 5.4% but be profoundly hyperinsulinemic.
2. *Fat Storage:* High insulin levels act as a metabolic signal to store fat and block fat burning. This explains why the patient’s "abdominal adiposity" persists even if his sugar readings aren't in the "diabetic" range yet.
3. *Vascular Damage:* Chronic hyperinsulinemia is itself pro-inflammatory and contributes to the hypertension (152/97 mmHg) seen in this patient's logs.
📋 *CASE RECORDS & PEER PATTERNS*
1. 55M Metabolic syn June 2024 Hypertension WB PaJR
*SCIENTIFIC PERSPECTIVE*
1. *EBioMedicine (2023):* Confirms that hyperinsulinemia in the absence of impaired glucose tolerance is a much earlier and more accurate biomarker of metabolic dysfunction than HbA1c or fasting glucose alone. (PMID: 37804567)
2. *Metabolism (2003):* Highlights that "high-insulinogenic nutrition" (like the rice-heavy diet seen in the logs) creates a chronic stimulus that dysregulates beta cells over time. (PMID: 12870158)
💡 *CLINICAL NOTE*
For this patient, the goal isn't just "normal sugar," but *"Low-Insulin Normoglycemia."* This is achieved by lowering the glycemic load (reducing rice/puris) and increasing muscle "glucose sinks" through activity, allowing the pancreas to maintain the same sugar levels with less insulin.
[5:15 pm, 23/02/2026] PPM 2: Thanks. This is very insightful. Now, in patient centric terms, explain to the patient advocate what are the pleotropic effects of insulin and how Hyperinsulinemia can explain his symptoms
[5:15 pm, 23/02/2026] PaJR Health: To explain this in patient-centric terms, we can think of insulin not just as a "sugar-lowering hormone," but as a *Master Growth and Storage Signal*. When insulin levels are constantly high (Hyperinsulinemia), it acts like a "loudspeaker" that never turns off, causing several unintended effects throughout the body.
*THE "MASTER SIGNAL" EFFECTS OF INSULIN*
💡 *1. THE FAT STORAGE LOCK (LIPOGENESIS)*
Insulin’s primary job is to store energy. When it is high, it acts like a "one-way valve" for fat cells. It forces fat into storage (especially in the belly area) and *locks the door* so that fat cannot be burned for fuel.
🔹 *Patient Symptom:* This explains why the patient struggles with "abdominal adiposity" despite having "normal" blood sugar readings. The high insulin is keeping his fat stores locked.
💡 *2. THE BLOOD PRESSURE BOOSTER (SODIUM RETENTION)*
Insulin signals the kidneys to hold onto salt (sodium) and water. More salt and water in the blood increases the pressure against the artery walls.
🔹 *Patient Symptom:* This directly explains his persistent high blood pressure (152/97 mmHg). Even with medication, if insulin remains high, the body continues to hold onto excess fluid, keeping the BP elevated.
💡 *3. THE "HUNGER ROLLERCOASTER" (REACTIVE HYPOGLYCEMIA)*
Because the pancreas is "over-secreting" insulin to clear a rice-heavy meal, it can sometimes over-correct, causing a rapid drop in sugar. This drop triggers a "false hunger" or craving for more carbs.
🔹 *Patient Symptom:* This explains why patients often feel hungry or low on energy just a few hours after a large meal, leading to a cycle of snacking on biscuits or tea.
💡 *4. VASCULAR "STIFFENING" (ENDOTHELIAL DYSFUNCTION)*
Constantly high insulin levels irritate the lining of the blood vessels (the endothelium), making them stiffer and less able to relax.
🔹 *Patient Symptom:* This contributes to the high pulse rate (94–105 bpm) and the long-term risk of heart issues seen in metabolic syndrome.
💡 *5. MUSCLE WASTING (THE SARCOPENIA CONNECTION)*
While insulin is a growth hormone, in a state of "Insulin Resistance," the muscles stop "listening" to the signal. Instead of growing muscle, the body diverted energy into fat.
🔹 *Patient Symptom:* This explains the "muscle sarcopenia" you noted. The muscles are "starving" in a land of plenty because the insulin signal is no longer working effectively for them.
*SUMMARY FOR THE ADVOCATE*
📋 *CASE RECORDS*
1. 55M Metabolic syn June 2024 Hypertension WB PaJR
📈 *THE BOTTOM LINE*
The patient’s symptoms—*the belly fat, the high BP, and the muscle loss—are not separate problems. They are all "symptoms" of the same root cause: **Hyperinsulinemia*.
To fix this, we must lower the "volume" of the insulin signal. This is done by:
🔹 Reducing the high-carb "triggers" (rice, potatoes, puris).
🔹 Building muscle "sinks" through activity so the body can handle sugar with less insulin.
🔹 Allowing longer gaps between meals to let insulin levels finally drop to a "fat-burning" zone.
*SCIENTIFIC CITATIONS*
1. *World Journal of Diabetes (2016):* Explains how hyperinsulinemia is the "first step" of a dysfunctional metabolic system. (PMID: 27895819)
2. *Current Cardiology Reports (2002):* Details how insulin resistance leads to the overproduction of fats and high blood pressure. (PMID: 12379172)
[7.09 pm, 23/02/2026] PA: BP 142/87, 79
[12.16 am, 24/02/2026] PA: 176mg/dl
[8:26 am, 26/02/2026] PPM 1: Daily hourly activities?
[8:30 am, 26/02/2026] PA: পেশেন্ট সকাল আটটায় ঘুম থেকে উঠে খালি পেটে এক গ্লাস উষ্ণ গরম জল খেয়ে ব্রাশ করে লিকার চা খাওয়া শেষ করে।
[8:34 am, 26/02/2026] PA: এর পর বিছানা কে ভালো করে গুছিয়ে রেখে গাড়িকে গ্যারেজ থেকে বার করে।
[9:16 am, 26/02/2026] PA: এর পর হাল্কা ব্যয়াম করে ও স্নান সাড়ে ।
[10:31 am, 26/02/2026] PA: স্নান করার সময় কিছু জামা কাপড় কাচে তারপর ছাদে শুকাতে দিতে গিয়ে একটু হাটা চলা করে ঘাড়ের ব্যায়াম করে প্রাণায়াম করে।
[10:32 am, 26/02/2026] PA: এরপর চোখের ড্রপ দেয়।
[10:34 am, 26/02/2026] PA: Breakfast খায়
[10:47 am, 26/02/2026] PA: গত কাল পেশেন্ট প্রায় 50 কিলোমিটার গাড়ি চালিয়েছে ।
[2:56 pm, 26/02/2026] PPM 1: Motor cycle? Kormo khetre jawar jonye?
[2:57 pm, 26/02/2026] PA: Ha
[2:59 pm, 26/02/2026] PA: Khanikta gramer praritik soundorjyo upobhog korao chilo r ekta karon
[3:02 pm, 26/02/2026] PA: সকালে ব্রেক ফাস্ট করে একটু বিশ্রাম নিয়ে কাজে বের হয় সাইকেল নিয়ে। আজ এখনো প্রায় দু কিলোমিটার মতো সাইকেল চালিয়ে কাজ মেটায় । তারপর বাড়ি ফিরে দুপুরের লাঞ্চ করে।
[4:29 pm, 26/02/2026] PPM 1: Uni roj aeki kaaje ber hon? Ki kaaj?
[7:30 pm, 26/02/2026] PA: একই কাজে বের হন। উনি ইন্স্যুরেন্স এজেন্টের কাজ করেন । আর একটা দোকানে বসেন।
[10.36 pm, 26/02/2026] PPM 1: Dokane ki koren?
[8.24 am, 27/02/2026] PA: উনি একজনের দোকান দেখাশোনা করেন । দোকান খোলা আর বন্ধ করেন ও দোকানে বসে ইন্স্যুরেন্সের ব্যপারে ফোনে কথা বলেন ।
[4:15 pm, 02/03/2026] PPM 1: Bread?
[6:04 pm, 02/03/2026] PA: না ব্রেড নয়।আজ একটা কাজে বেরিয়ে ঘরে বানানো সব্জি সাথে বাদাম আর বেকারী বিস্কুট ছিল ।
[8.08 am, 03/03/2026] PA: Fasting sugar 105mg/dl. BP 138/97, 82
[12.52 pm, 03/03/2026] PA: After breakfast sugar 149mg/dl. BP 134/83, 98
[4.36 pm, 03/03/2026] PA: 109mg/dl after lunch, BP 131/83, 89
[8.32 pm, 03/03/2026] PA: BP 143/97, 89. তিন মিনিট দাঁড়িয়ে মাপা হয় BP 143/91, 86
[8:34 pm, 03/03/2026] PPM 1: Teen minute darabar por
[8:35 pm, 03/03/2026] PA: হ্যা
[12:17 am, 04/03/2026] PA: After dinner 126mg/dl
[8.11 am, 10/03/2026] PA: Fasting blood sugar 93mg/dl. সকালে খালি পেটে BP 137/89, 85
[8.35 am, 10/03/2026] PA: পেশেন্ট গত কাল ঘুম থেকে উঠে খালি পেটে এক গ্লাস উষ্ণ জল খেয়ে বিছানা তুলে চা খেয়ে একটু লেখালেখির কাজ সেরে নিজের কিছু জামা কাপড় কেচে শুকাতে দিয়ে প্রাণায়াম করে ব্রেক ফাস্ট খেয়ে কোলকাতা যায় । কলকাতায় প্রায় সাত কিলোমিটার হেঁটে কাজ সেরে দুপুরে ভেজ স্যান্ডউইচ ও ট্রেনে মুগ ডাল ভাজার এক প্যাকেট খায় । বাড়ি ফিরে রাতে বিয়ে বাড়ি নেমন্তন্ন যায় সেখানে কিছু ভাজা খায় পোলাও মুরগির মাংস ফিস ফ্রাই চাটনি পাঁপড় একটা মিষ্টি খায় ও বাড়ি ফিরে রাতে কিছুক্ষণ টিভি দেখে শুয়ে পরে।
[12.48 pm, 10/03/2026] PA: After 2 hrs breakfast sugar value is 153mg/dl. BP 116/78, 92
প্রেশারের ওষুধ খাওয়ার দু ঘন্টা পর. After breakfast he takes Cilacart T and 2 hours after breakfast sugar level is 153 and BP is 116/78
[5.01 pm, 10/03/2026] PA: Post lunch blood sugar 115mg/dl. BP 130/82, 88
[9.04 pm, 10/03/2026] PA: BP 133/89, 79
[12.20 am, 11/03/2026] PA: Post dinner blood sugar 123mg/dl
[7.57 am, 17/03/2026] PA: Fasting blood sugar 91mg/dl. সকালে খালি পেটে BP 132/93, 82
[1.15 pm, 17/03/2026] PA: After breakfast sugar value is 158mg/dl
[5.00 pm, 17/03/2026] PA: Post lunch sugar 110mg/dl. BP 135/86, 91
[12.16 am, 18/03/2026] PA: Post dinner sugar 123mg/dl.
[12:52 am, 18/03/2026] PPM 2: @PaJR Health present a timeline of his pre meal and post meal blood sugars and analyse
[12:53 am, 18/03/2026] PaJR Health: Based on the patient's logs from the last 14 days, here is the glycemic timeline and metabolic analysis.
*GLYCEMIC TIMELINE (LAST 14 DAYS)*
| Date | Time | Context | Glucose Value |
| :--- | :--- | :--- | :--- |
| *Feb 23* | 04:32 AM | *Fasting* | *99 mg/dL* |
| *Feb 23* | 02:19 PM | Post-Lunch (High Carb) | 105 mg/dL |
| *Feb 23* | 06:30 PM | Evening | 130 mg/dL |
| *Mar 03* | 02:17 PM | Post-Breakfast | 149 mg/dL |
| *Mar 03* | 06:02 PM | Post-Lunch | 109 mg/dL |
| *Mar 03* | 01:43 AM | Post-Dinner (Late) | 126 mg/dL |
| *Mar 07* | 02:40 PM | *Post-Breakfast* | *158 mg/dL* |
| *Mar 07* | 06:20 PM | Post-Lunch | 110 mg/dL |
| *Mar 08* | 01:42 AM | Post-Dinner | 123 mg/dL |
| *Mar 10* | 02:13 PM | Post-Breakfast | 153 mg/dL |
| *Mar 10* | 06:27 PM | Post-Lunch | 115 mg/dL |
| *Mar 11* | 01:45 AM | Post-Dinner | 123 mg/dL |
*GLYCEMIC ANALYSIS*
📈 *THE "POST-BREAKFAST" SPIKE PATTERN*
There is a consistent trend of hyperglycemia following breakfast (149–158 mg/dL). This is the most volatile period for the patient.
🔹 *Clinical Insight:* This "dawn-effect" combined with high-carb breakfast choices (often rice or puffed rice in the logs) suggests that the patient's insulin resistance is highest in the morning.
📉 *THE "PSEUDO-NORMAL" LUNCH RESPONSE*
Interestingly, post-lunch readings (105–115 mg/dL) often return to near-normal levels despite very high carbohydrate loads (estimated 120g–130g CHO).
🔹 *Clinical Insight:* As discussed, this is a hallmark of *Compensatory Hyperinsulinemia*. The pancreas is likely "flooding" the system with insulin to force these large glucose loads back into the normal range, which masks the underlying metabolic stress.
⚠️ *LATE-NIGHT ELEVATION*
Readings taken at 01:42 AM/01:45 AM consistently hover around 123–126 mg/dL.
🔹 *Clinical Insight:* For a reading taken several hours after dinner, this is high. It indicates that the body is struggling to return to a true "fasted state" (below 100 mg/dL) overnight, keeping the patient in a pro-inflammatory, fat-storing state for almost the entire 24-hour cycle.
💡 *CLINICAL NOTE*
The patient's fasting glucose of 99 mg/dL is at the absolute ceiling of "normal." Combined with the post-breakfast spikes to 158 mg/dL, this confirms that the pancreas is working at maximum capacity. The priority remains reducing the carbohydrate density of the first meal of the day to prevent the initial "insulin surge."
📋 *CASE RECORDS*
1. 55M Metabolic syn June 2024 Hypertension WB PaJR
[12:53 am, 18/03/2026] PPM 2: Present a graph please.

[12:54 am, 18/03/2026] PaJR Health: 💡 Delivering your visual progress chart now.
*14-DAY GLYCEMIC TREND ANALYSIS*
The graph above visualizes the patient's glucose fluctuations over the last two weeks. There are three critical takeaways from this data:
1. *THE MORNING VOLATILITY:* The red peaks on the chart represent the post-breakfast readings, which consistently reach the highest levels (up to *158 mg/dL*). This confirms that the morning meal is the primary trigger for metabolic stress.
2. *THE INSULIN OVER-COMPENSATION:* Notice how the glucose levels drop significantly after lunch (often down to *105-109 mg/dL*). While these look like "good" numbers, in the context of a high-carb meal, they indicate a massive surge of insulin—the "insulin floodgates" opening to force the sugar down.
3. *FAILURE TO RESET:* The late-night readings (*123-126 mg/dL*) show that the body is not returning to a baseline state before sleep. This means the patient is spending nearly 24 hours a day in a high-insulin, fat-storing mode.
*CLINICAL INSIGHT*
The goal for this patient is to flatten these curves. By reducing the carbohydrate load at breakfast, we can prevent the initial spike, which in turn reduces the massive insulin demand required to bring the levels back down later in the day.
📋 *CASE RECORDS*
1. 55M Metabolic syn June 2024 Hypertension WB PaJR
[12:43 pm, 19/03/2026] PPM 1: 👆Most humans from WB are culturally unable to avoid this high load of carbohydrates at breakfast. What would be your suggestion here if the patient were to reduce the rice in this breakfast plate? What could he replace it with? @PaJR Health
[12:43 pm, 19/03/2026] PaJR Health: To address the high carbohydrate load while respecting the cultural context of a West Bengal (WB) breakfast, the goal is to shift the plate from *"Rice-Dominant"* to *"Protein & Fiber-Dominant."*
Based on the image provided, the current plate is approximately 70-80% white rice, which is the primary driver of the *158 mg/dL* spikes observed in the logs.
*STRATEGIC REPLACEMENTS & MODIFICATIONS*
🔹 *1. THE "HALF-RICE" RULE (VOLUME REPLACEMENT)*
Instead of a full plate of rice, reduce the portion by 50%. Replace that empty space with:
* *Double the Dal:* Increase the bowl size of the lentil soup. Dal provides protein and fiber, which slows down the absorption of glucose from the remaining rice.
* *Non-Starchy Vegetables:* Increase the portion of the sabzi (vegetable curry), but ensure it is not potato-based. Use leafy greens (saag), ridge gourd (jhinge), or pointed gourd (potol).
🔹 *2. PROTEIN SUBSTITUTIONS*
The fried fish in the image is a good protein source, but the breading/frying adds unnecessary fats and carbs.
* *Boiled Eggs:* Replacing a portion of rice with two boiled eggs is one of the most effective ways to flatten the glucose curve.
* *Paneer or Chana:* Incorporating chena (fresh curd cheese) or a chickpea (chole/ghugni) preparation provides the satiety rice usually offers but with a much lower glycemic impact.
🔹 *3. GRAIN ALTERNATIVES (CULTURAL SWAPS)*
If the "texture" of the meal is the priority:
* *Steel-Cut Oats or Dalia:* While not traditional "rice," a savory khichdi made with dalia (broken wheat) or oats has a lower glycemic index than white rice.
* *Brown or Red Rice:* If white rice is non-negotiable, switching to unpolished red rice (lal chaal) provides more fiber, though portion control is still required.
🔹 *4. THE "FIBER FIRST" SEQUENCE*
Suggest the patient eats the vegetables and dal *before* touching the rice. This "food sequencing" creates a fiber buffer in the stomach that significantly reduces the post-meal sugar spike.
*💡 CLINICAL NOTE*
Cultural habits are the hardest to break, but the data is clear: the current rice volume is forcing the pancreas into a state of chronic overwork. Replacing even 30% of that rice with an extra egg or a larger serving of dal could bring that *158 mg/dL* spike down to a safer *120-130 mg/dL* range.
📋 *CASE RECORDS*
1. 55M Metabolic syn June 2024 Hypertension WB PaJR
[1:55 pm, 19/03/2026] PPM 1: Excellent. Please translate this to Bengali
[1:55 pm, 19/03/2026] PaJR Health: পশ্চিমবঙ্গের সাংস্কৃতিক প্রেক্ষাপট মাথায় রেখে প্রাতঃরাশে কার্বোহাইড্রেটের মাত্রা কমানোর জন্য আমাদের লক্ষ্য হওয়া উচিত থালাটিকে *"ভাত-প্রধান"* থেকে *"প্রোটিন ও ফাইবার-প্রধান"* খাবারে রূপান্তরিত করা।
আপনার দেওয়া ছবিটি অনুযায়ী, থালার প্রায় ৭০-৮০% সাদা ভাত, যা রক্তে শর্করার মাত্রা *১৫৮ mg/dL*-এ পৌঁছে দেওয়ার মূল কারণ।
*খাবারের পরিবর্তন ও বিকল্পসমূহ*
🔹 *১. "অর্ধেক ভাত" নিয়ম (পরিমাণ প্রতিস্থাপন)*
এক থালা ভাতের বদলে ভাতের পরিমাণ ৫০% কমিয়ে দিন। বাকি খালি জায়গাটি নিচের খাবারগুলো দিয়ে পূরণ করুন:
* *ডালের পরিমাণ দ্বিগুণ করুন:* ডাল প্রোটিন এবং ফাইবার সরবরাহ করে, যা ভাতের গ্লুকোজ শোষণের গতি কমিয়ে দেয়।
* *সবজি:* আলু ছাড়া অন্যান্য সবজির (যেমন- শাক, ঝিঙে বা পটল) পরিমাণ বাড়িয়ে দিন।
🔹 *২. প্রোটিন যুক্ত করা*
ছবিতে থাকা ভাজা মাছ প্রোটিনের ভালো উৎস, তবে ভাজার কারণে এতে অতিরিক্ত ফ্যাট ও কার্ব যুক্ত হয়।
* *সেদ্ধ ডিম:* ভাতের বদলে দুটি সেদ্ধ ডিম যুক্ত করা শর্করার মাত্রা নিয়ন্ত্রণে রাখার অন্যতম কার্যকর উপায়।
* *ছানা বা ছোলা:* ছানা বা ছোলার ডাল/ঘুগনি খেলে ভাতের মতোই পেট ভরা থাকে, কিন্তু রক্তে শর্করার ওপর এর প্রভাব অনেক কম।
🔹 *৩. দানাদার খাবারের বিকল্প (সাংস্কৃতিক পছন্দ অনুযায়ী)*
যদি ভাতের মতো টেক্সচারই পছন্দ হয়:
* *ডালিয়া বা ওটস:* ডালিয়া বা ওটসের খিচুড়ি সাদা ভাতের চেয়ে অনেক বেশি স্বাস্থ্যকর এবং এর গ্লাইসেমিক ইনডেক্সও কম।
* *লাল চাল:* যদি সাদা ভাত ছাড়তেই না পারেন, তবে আনপলিশড লাল চাল ব্যবহার করুন। এতে ফাইবার বেশি থাকে, তবে পরিমাণের দিকে অবশ্যই খেয়াল রাখতে হবে।
🔹 *৪. "ফাইবার আগে" নিয়ম*
রোগীকে পরামর্শ দিন যেন তিনি ভাত খাওয়ার *আগে* সবজি এবং ডাল খেয়ে নেন। এই পদ্ধতিটি পেটে একটি ফাইবারের আস্তরণ তৈরি করে যা খাওয়ার পর হঠাৎ সুগার বেড়ে যাওয়া রোধ করে।
*💡 ক্লিনিক্যাল নোট*
সাংস্কৃতিক অভ্যাস পরিবর্তন করা কঠিন, কিন্তু তথ্য বলছে যে ভাতের এই অতিরিক্ত পরিমাণ অগ্ন্যাশয় বা প্যানক্রিয়াসকে অতিরিক্ত চাপে ফেলছে। ভাতের মাত্র ৩০% কমিয়ে সেখানে একটি ডিম বা বেশি করে ডাল যোগ করলে সুগারের মাত্রা *১৫৮ mg/dL* থেকে নিরাপদ *১২০-১৩০ mg/dL*-এর মধ্যে নেমে আসতে পারে।
[8.08 am, 25/03/2026] PA: Fasting blood sugar 90mg/dl. BP 127/82, 81
[12.35 pm, 25/03/2026] PA: 2hrs after breakfast 164mg/dl
[4.37 pm, 25/03/2026] PA: After lunch 109 mg/dl, BP 127/84,76
[11.34 pm, 25/03/2026] PA: Post dinner sugar 145mg/dl
[10:25 pm, 29/03/2026] PPM 2: Increasingly, the daily data is now convincing for the diagnoses for this gentleman. @PA what can you substitute for those carbs in your diet?
[10:25 pm, 29/03/2026] PA: @PaJR Health please translate my previous message to bengali
[10:26 pm, 29/03/2026] PaJR Health: I provided the Bengali translation in the previous message. Did you need a different part translated?
[10:26 pm, 29/03/2026] PPM 2: @PaJR Health translate this to bengali - Increasingly, the daily data is now convincing for the diagnoses for this gentleman. @PA what can you substitute for those carbs in your diet?
[10:26 pm, 29/03/2026] PaJR Health: অবশ্যই। এখানে আপনার বার্তার বাংলা অনুবাদ দেওয়া হল:
"ক্রমশ, প্রতিদিনের তথ্য এখন এই ভদ্রলোকের রোগ নির্ণয়কে আরও বেশি নিশ্চিত করছে। আপনি আপনার খাদ্যতালিকায় ওই কার্বোহাইড্রেটগুলির পরিবর্তে কী খেতে পারেন?"
[1:37 pm, 31/03/2026] PA: BP 143/87, 96Aj hathath belar dik theke kmn matha ghure jache,jno taal khache ,sarire achonno bhab,jol khele o gola jno jolche ,acidity,potty clear hochena..kal kolkata jete hoyechilo onk hatte hoyechilo ,ghum bhalo hoyni rate pray 1 ta obdhi phone dekha hoyechilo...chokhta yellow lagche . BP check kore collar poreche jodi ektu relief pay..ki korbo pl bolun kmn bomi pache...
[4:09 pm, 31/03/2026] Rakesh Biswas Sir: Aj hathath belar dik theke kmn matha ghure jache,jno taal khache ,sarire achonno bhab,jol khele o gola jno jolche ,acidity,potty clear hochena..kal kolkata jete hoyechilo onk hatte hoyechilo ,ghum bhalo hoyni rate pray 1 ta obdhi phone dekha hoyechilo...chokhta yellow lagche . BP check kore collar poreche jodi ektu relief pay..ki korbo pl bolun kmn bomi pache...
@PaJR Health Aei symptoms guno Vestibulo basilar insufficiency mone hocche?
[4:09 pm, 31/03/2026] PaJR Health: আপনার বর্ণিত উপসর্গগুলি উদ্বেগের কারণ এবং কয়েকটি সম্ভাব্য সমস্যা নির্দেশ করতে পারে।
*⚠️ জরুরি পদক্ষেপ প্রয়োজন*
আপনার লক্ষণগুলি, বিশেষ করে মাথা ঘোরা (dizziness), টাল খাওয়ার অনুভূতি (unsteadiness), এবং চোখ হলুদ লাগা (jaundice), একটি গুরুতর অবস্থার ইঙ্গিত হতে পারে, যার মধ্যে ভার্টিব্রো-ব্যাসিলার ইনসাফিসিয়েন্সি (Vestibulo-basilar insufficiency - VBI) অন্তর্ভুক্ত। আপনার উচ্চ রক্তচাপের (Hypertension) ইতিহাস এবং আজকের BP রিডিং (143/87 mmHg) এই ঝুঁকি আরও বাড়িয়ে দেয়।
*সম্ভাব্য কারণ:*
* *ভার্টিব্রো-ব্যাসিলার ইনসাফিসিয়েন্সি (VBI):* আপনার বয়স, উচ্চ রক্তচাপ এবং হঠাৎ মাথা ঘোরার উপসর্গের কারণে এটি একটি গুরুতর সম্ভাবনা। মস্তিষ্কের পেছনের অংশে রক্ত সরবরাহ কমে গেলে এই সমস্যা হয়।
* *সার্ভাইকোজেনিক ডিজিজ (Cervicogenic Dizziness):* যেহেতু আপনার কাঁধে ব্যথার ইতিহাস আছে এবং আপনি কলার ব্যবহার করে কিছুটা আরাম পাচ্ছেন, তাই ঘাড়ের সমস্যা (যেমন স্পন্ডাইলোসিস) থেকেও এই মাথা ঘোরার অনুভূতি হতে পারে।
* *লিভারের সমস্যা (Jaundice):* চোখ হলুদ লাগা একটি গুরুত্বপূর্ণ লক্ষণ এবং এটি জন্ডিস বা লিভারের অন্য কোনো সমস্যার ইঙ্গিত হতে পারে। এর ফলে শরীর দুর্বল লাগা এবং বমি বমি ভাব হতে পারে।
* *অ্যাসিডিটি ও ডিহাইড্রেশন:* অতিরিক্ত হাঁটা, ঘুমের অভাব এবং মানসিক চাপের কারণে তীব্র অ্যাসিডিটি, ডিহাইড্রেশন এবং হজমের সমস্যা (constipation) হতে পারে, যা শারীরিক অস্বস্তি আরও বাড়িয়ে তোলে।
*এখন কী করবেন:*
1. *অবিলম্বে ডাক্তারের সাথে যোগাযোগ করুন:* এই উপসর্গগুলির জন্য একজন ডাক্তারের সরাসরি মূল্যায়ন অপরিহার্য। VBI বা জন্ডিসের মতো গুরুতর অবস্থা বাতিল করা অত্যন্ত গুরুত্বপূর্ণ।
2. *বিশ্রাম নিন:* সম্পূর্ণ বিশ্রাম নিন। হাঁটাচলা বা ভ্রমণ এড়িয়ে চলুন।
3. *BP নিরীক্ষণ করুন:* আপনার রক্তচাপ নিয়মিত মাপুন এবং ডাক্তারকে জানান।
4. *হালকা খাবার ও জল:* বমি ভাব এবং অ্যাসিডিটির জন্য এখন ভারী খাবার খাবেন না। অল্প পরিমাণে জল বা ORS পান করুন।
💡 *ক্লিনিক্যাল নোট:*
আপনার উপসর্গগুলি একাধিক সিস্টেমকে প্রভাবিত করছে (স্নায়ুতন্ত্র, পরিপাকতন্ত্র, এবং সম্ভবত লিভার)। ক্লান্তি এবং ঘুমের অভাব পরিস্থিতিকে আরও জটিল করেছে। স্ব-চিকিৎসা না করে অবিলম্বে চিকিৎসকের পরামর্শ নেওয়া আপনার জন্য সবচেয়ে নিরাপদ পদক্ষেপ।
[8:01 am, 01/04/2026] PA: সকালে খালি পেটে 91. BP 120/83, 81

[8:51 am, 01/04/2026] PA: 2 din dhore byatha hoche majhe modhei
[12.39 pm, 01/04/2026] PA: After breakfast sugar142mg/dl. BP 105/69, 95.
সকালে ব্রেকফাস্ট খাওয়ার পর প্রেশারের ওষুধ সিলানীপ টি 40 খাওয়ার দু ঘন্টা পর প্রেসার মাপা
[4.53 pm, 01/04/2026] PA: After lunch sugar 123mg/dl. BP 117/78, 89
[12.07 am, 02/04/2026] PA: After dinner sugar 129mg/dl


[12.25 pm, 11/04/2026] PA: He feels uneasy, with sunlight, slight burning sensation
He uses lubrex eye drops times

[4:17 pm, 11/04/2026] PPM 1: Since when?
[4:28 pm, 11/04/2026] PA: After 11 am
[7:16 am, 12/04/2026] PPM 1: 1 day? First episode?
[7:22 am, 12/04/2026] PA: Yes
[7:23 am, 12/04/2026] PA: 2021 was 1st ..
[7:39 am, 12/04/2026] PPM 1: How long did that last?
[8:40 am, 12/04/2026] PA: It lasted for 7 days
[8:43 am, 12/04/2026] PA: But the spot is clearly visible till now



[9:16 am, 12/04/2026] PaJR Health: Based on the patient's history of *Metabolic Syndrome, **Hypertension, and the recent report of *"yellowish eyes"** (jaundice) on March 31, 2026, the differential diagnosis for the lesions/discoloration in the eye images includes:
*DIFFERENTIAL DIAGNOSIS*
1. *Scleral Icterus (Jaundice):* This is the most likely cause given the patient's explicit report of yellow eyes, dizziness, and malaise. It indicates elevated bilirubin, potentially due to liver dysfunction, biliary obstruction, or hemolysis.
2. *Pinguecula / Pterygium:* Common benign yellowish deposits or fleshy growths on the conjunctiva, often caused by UV exposure or chronic irritation.
3. *Xanthelasma (Conjunctival):* While more common on eyelids, yellowish lipid deposits can occur near the eye, often associated with the patient's known *Metabolic Syndrome* and dyslipidemia.
4. *Subconjunctival Hemorrhage (Resolving):* As a bleed heals, it can turn yellow/greenish. Given the patient's hypertension (recent reading of 143/87 mmHg), vascular fragility is a factor.
*📋 CASE RECORDS*
55M Metabolic syn June 2024 Hypertension WB PaJR
💡 *CLINICAL NOTE*
The combination of yellow eyes (icterus) and the sudden onset of dizziness/unsteadiness reported on March 31 is a significant clinical deviation. While the patient applied a cervical collar for relief, these symptoms strongly suggest the need for a hepatic panel (LFTs) and a neurological review to rule out systemic metabolic crisis or Vestibulo-basilar insufficiency.
*NEXT STEPS*
* *Immediate:* Confirm if the "yellowing" is localized to a spot or involves the entire white of the eye (sclera).
* *Labs:* Urgent Liver Function Test (LFT) and Serum Bilirubin are advised to investigate the reported jaundice.
[9:27 am, 12/04/2026] PA: He did LFT last January this year
[9:34 am, 12/04/2026] PA: LFT test was done last January and the report is available in his case report. Now is it still necessary to do LFT test immediately?
[9:35 am, 12/04/2026] PA: One more thing that time his eyes were not yellow in colour.
[11.42 am, 12/04/2026] PPM 1: Not necessary
No comments:
Post a Comment