
THIS IS AN ONLINE E LOG BOOK TO DISCUSS OUR PATIENT'S DE-IDENTIFIED HEALTH DATA SHARED AFTER TAKING HER SIGNED INFORMED CONSENT. HERE WE DISCUSS OUR PATIENT'S PROBLEMS THROUGH SERIES OF INPUTS FROM AVAILABLE GLOBAL ONLINE COMMUNITY EXPERTS WITH AN AIM TO SOLVE THOSE PATIENT'S CLINICAL PROBLEMS WITH COLLECTIVE CURRENT BEST EVIDENCE BASED INPUTS.
PREVIOUS HISTORY OF THE PATIENT AVAILABLE IN THE BELOW TWO LINKS 👇 AND ALSO ARCHIVED IN THE PRESENT BLOG.
43F Patient came to OPD with C/O Bilateral pedal edema since 1 month.
Patient was apparently asymptomatic till 1 month ago, then she developed c/o B/L pedal edema (pitting type, extending upto the knee) and chest discomfort (now subsided) now patient has c/o tingling of Rt. Upper Limb.
Patient has come for regular checkup of HTN and DM
Had h/o UTI 1 month ago.
Numbness in Rt. upper limb and Rt. lower limb since 1 month.
PAST HISTORY: k/c/o Diabetes since 10 yrs and is on Insulin HAI 15U-20U-25U
k/c/o Hypothyroidism since 6 yrs and is on Tab. Thyroxine 125mg PO/OD
k/c/o Hypertension since 2 yrs and Tab. Cilnidipine 10mg+Tab. Metoprolol 50mg PO/OD+ Tab. Olmesartan 70mg PO/OD
N/K/C/O CAD, CVA, TB, Asthma, Epilepsy.
PERSONAL HISTORY: Normal appetite, mixed diet, inadequate sleep, normal bladder and bowel movement, no addiction. FAMILY HISTORY: Not significant
FAMILY HISTORY: Not significant

GENERAL EXAMINATION: The patient was examined in well lit room after taking her consent.
The patient was conscious, coherent and co-operative. She was well oriented to time, place and person.


ON EXAMINATION: The patient is conscious, coherent and cooperative.
BP - 160/90
Temp - 97.2F
Pulse - 88 BPM
RR - 18
SYSTEMIC EXAMINATION:
CVS - S1, S2 heard, no murmurs
CNS - NFND
RS - BAE+, NVBS
P/A - Soft, Non tender, No organomegaly
INVESTIGATIONS:
Serology -






PLBS 346mg/dl
DIET -
08/10/2023
Time values Medication Food +Quantity
(mg/dl) (gm)
8 am 140 Metformin 500mg Wheat rawa 150
Glimiperide 1mg 150
Nicardia 20mg
Thyronorm 125mcg

1 pm 181 Metformin 500mg Foxtail millets
Nicardia 20mg Millets
Thyronorm 125mcg 100gms


3 pm 170
8 pm 176 Metformin 500mg Wheat Upma
Nicardia 20mg 100gms
10 pm Missed
09/10/2023
Time Values Medication Food + Quantity
8 am 207mg/dl Metformin 500mg Ragi dosa
Glimiperide 1 mg 100gms
Nicardia 20mg
Thyronorm 125mcg

10 am Missed
1 pm 194mg/dl Metformin 500mg Arekalu
Nicardia 20 mg Millets
Thyronorm 125mcg 100gms

8 pm 205mg/dl Metformin 500mg Millets
Nicardia 20mg Dosa
100gms

10/10/2023
Time Values Medications Food Quantity
9 am 172mg/dl Metformin 500mg Fruits apple
Glimiperide 1mg Pomegranate
Nicardia 20mg 120gms
Frusemide 20 mg
Thyronorm 125mcg

1 pm 164mg/dl Metformin 500mg Millets
Nicardia 20mg Red sorrel
Thyronorm 125mcg 100gms
Frusemide 20mg

3 pm 199mg/dl
8 pm 155mg/dl Metformin 500mg Millets
Nicardia 20mg Dosa
100gms

11/10/2023
Time Values Medication Food + Quantity
 9 am 251mg/dl
9 am 251mg/dl
7 am 111mg/dl Metformin 500mg Idly
Glimiperide 1mg
Nicardia 20mg 100gms
Frusemide 20mg
Thyronorm 125mcg

BP Readings
Date mmhg
08-10-2023 152/79
09-10-2023 167/84
10-10-2023 163/88
11-10-2023 155/81
12-10-2023 154/80
13-10-2023 161/86
14-09-2023 172/98
15-10-2023 154/96
17-10-2023 177/98
20-10-2023 170/94
NOVEMBER 09, 2024
 After food
After food
 At 1 pm
At 1 pm

 PPM 1: What is the vial shown here?
PPM 1: What is the vial shown here?
[05-11-2024] PPM 1: Reviewing her in OPD now.
EMR SUMMARY
Age/Gender : 45 Years/Female
Discharge Type: Relieved
Admission Date: 21/10/2024 01:32 PM
Diagnosis
- ACUTE PULMONARY PEDEMA SECONDARY TO CKD WITH DIABETIC NEPHROPATHY
- HEART FAILURE WITH PRESERVED EJECTION FRACTION(EF56%)
- WITH ANEMIA OF CHRONIC DISEASE
- K/C/O DM2 SINCE 15 YRS
- K/C/O HTN SINCE 10 YRS
- K/C/O HYPOTHYROIDISM SINCE 1YR
Case History and Clinical Findings
- PT WAS BROUGHT TO THE CASUALTY WITH C/O BREATHLESSNESS SINCE 2 DAYS
- HOPI: PT WAS APPARENTLY NORMAL 2 DAYS BACK THEN SHE DEVELOPED BREATHLESSNESS GRADE 2 MMRC INITIALLY AND GRADUALLY PROGRESSED TO GRADE 4 ASSOCIATED WITH COUGH WITH EXPECTORATION - GREENISH MUCOID SPUTUM SINCE 4 DAYS.
- FEVER SINCE 4 DAYS-HIGH GRADE, INTERMITTENT, ASSOCIATED WITH CHILLS AND RIGORS AND RELIEVED BY MEDICATION
- C/O B/L SWELLING OF LOWER LIMBS - PITTING TYPE, EXTENDED UPTO THE KNEE SINCE 1 YR (ON AND OFF)
- C/O DECREASED URINE OUTPUT SINCE 1 YR - VERY MUCH REDUCED SINCE 3 DAYS
- C/O ABDOMINAL DISTENSION SINCE 4-5 MONTHS, ORTHOPNEA PRESENT
- NO C/O CHEST PAIN, PALPITATIONS, PND, SWEATING, GIDDINESS
- K/C/O DM2(SINCE 15 YRS) INITIALLY STARTED INSULIN BUT NOW ON OHAS - SITAGLIPTIN 50 & METFORMIN 1000 & GLIMIPERIDE2
- K/C/O HTN SINCE 10 YRS USING T.PRAZOSIN 5MG
- K/C/O HYPOTHYROIDISM SINCE 1 YR USING T.THYRONORM 150MCG
- K/C/O CKD SINCE 1 YR ON CONSERVATIVE MANAGEMENT
- NOT K/C/O CVA, CAD, TB, EPILEPSY, ASTHMA
- GENERAL EXAMINATION-PT IS C/C/C
- PALLOR, EDEMA PRESENT(PITTING TYPE), NO ICTERUS CYANOSIS LYMPHADENOPATHY
- BP-240/100MMHG
- PR112BPM RR42CPM
- SPO2 67% AT RA GRBS 100MG%
- SYSTEMIC EXAMINATION
- CVS: INSPECTION-JVP NOT RAISED, CHEST WALL SHAPE NORMAL AND SYMMETRICAL, NO DILATED VEINS/SCARS, KYPHOSCOLIOSIS ABSENT
- PALPATION - APICAL IMPULSE NORMAL NO PARASTERNAL HEAVE, NO THRILLS PERCUSSION - DULL NOTE PRESENT
- AUSCULTATION-S1S2 PRESENT, NO MURMURS
- RESPIRATORY SYSTEM: BAE PRESENT, NVBS, DIFFUSE CREBS PRESENT P/A: SOFT, NON TENDER, NO ORGANOMEGALY
- CNS: NO FOCAL NEUROLOGICAL DEFICITS
Course in Hospital
PT WAS BROUGHT TO CASUALTY ON 21/0/2024 AT 1:30 PM WITH H/O SEVERE SOB ON EXAMINATION PR 112 BPM, BP 240/ 100 MMHG, RR 42CPM,SPO2 61% AT RA, ON AUSCULATION DIFFUSE FINE CREPS PRESENT IN ALL LUNG FIELDS, IMMEDIATELY PT WAS GIVEN 10 LIT OF O2 GIVEN, INJ LASIX 80 MG IV STAT GIVEN, IMJ NTG 1CC IV STAT GIVEN, AND OBSERVED FOR 5 MINS WITH O2 SATURATION 90% AND PT KEPT ON CONTINUOUS CPAP AND PT SHIFTED TO ICU THERE PT GIVEN ANTIHYPERTENSIVE TREATMENT AND HYOOGLYCEMIC AGENTS AND KEPT UNDER OBSERVATION AND AT 5PM PT BP IS 190/100 MMHG, PR IS 98 BPM, RR 30 CPM, SATURATION 98% WITH CPAPA, DIFFUSE CREPS PRESENT ON ASCULATION AGAIN INJ NTG 1CC IV GIVEN AND LASIX 40 MG GIVEN AT 8 PM BP 180/100 MMHG PR 100BPM, RR 20 CPM AND SPO2 100 ON CPAP AND ADVISED INTERMITTENT CPAP WITH O2 SUPPORT WAS GIVEN.
ON 22/10/24 BP WAS 130/70MMHG, PR 86 RR 18 CPM SPO2 98% WITH 6 LIT O2 AND CONTINUED LASIX 40 MG BD GIVEN, PRAZOSIN 500MG, TAB.OLKEM TRIO, INJ AUGMENTIN 1.2 G, PT CONDITION IMPROVED AND WAS KEPT ON 4 LIT O2 AND CONTINUED SAME CONDITION ON 24 /10/2024 SAME TREATMENT WAS CONTINUED PT CONDITION IMPROVED ON AUSCULTATION B/L LUNG FEILDS ARE CLEARED AND CONTINUED ON INTERMITTENT O2 WITH NASAL PRONGD AT RATE OF 2 LIT/ MIN AND ADVISED DISCHARGE.
Investigation
Arterial Blood Gas (ABG):
- pH: 7.38
- PCO₂: 32.2
- PO₂: 158
- HCO₃: 19.0
- St. HCO₃: 20.3
- BEB: -5.0
- BEecf: -5.1
- TCO₂: 41.3
- O₂ Sat: 99.3
- O₂ Count: 9.5
Kidney Function Tests:
- Blood Urea:
- First Test: 70 mg/dL (Reference: 12-42 mg/dL)
- Second Test: 88 mg/dL
- Serum Creatinine:
- First Test: 1.9 mg/dL (Reference: 0.6-1.1 mg/dL)
- Second Test: 1: 2.0 mg/dL
- Third Test: 2: 1.5 mg/dL
Serum Electrolytes (Na, K, Cl):
First Test:
- Sodium: 130 mmol/L (Reference: 136-145 mmol/L)
- Potassium: 3.7 mmol/L (Reference: 3.5-5.1 mmol/L)
- Chloride: 101 mmol/L (Reference: 98-107 mmol/L)
Second Test:
- Sodium: 132 mmol/L
- Potassium: 3.5 mmol/L
- Chloride: 102 mmol/L
Third Test:
- Sodium: 134 mmol/L
- Potassium: 3.3 mmol/L
- Chloride: 103 mmol/L
Fourth Test:
- Sodium: 135 mmol/L
- Potassium: 3.6 mmol/L
- Chloride: 98 mmol/L
Liver Function Test (LFT):
- Total Bilirubin: 0.60 mg/dL
- Direct Bilirubin: 0.19 mg/dL
- SGOT (AST): 29 IU/L
- SGPT (ALT): 20 IU/L
- Alkaline Phosphatase: 110 IU/L
- Total Proteins: 5.8 gm/dL
- Albumin: 3.0 gm/dL
- A/G Ratio: 1.06
Hepatitis Screening:
- HBsAg (Rapid): Negative
- Anti-HCV Antibodies (Rapid): Non-Reactive
Complete Urine Examination (CUE):
- Color: Pale yellow
- Appearance: Clear
- Reaction: Acidic
- Specific Gravity: 1.010
- Albumin: ++
- Sugar: Nil
- Bile Salts: Nil
- Bile Pigments: Nil
- Pus Cells: 4-6
- Epithelial Cells: 2-3
- Red Blood Cells: Nil
- Crystals: Nil
- Casts: Nil
- Amorphous Deposits: Absent
- Others: Nil
Thyroid Profile:
- T3: 0.36 ng/mL
- T4: 15.17 µg/dL
- TSH: 5.4 µIU/mL
Treatment Given (Enter only Generic Name)
- INTERMITTENT C-PAPFLUID
- RESTRICTION LESS THAN 1LIT/DAY
- SALT RESTRICTION LESS THAN 2-3GMS/DAY
- INJ NTG 1CC IN 4ML NS ICC IV STAT
- INJ.LASIX 40MG IV BD
- INJ.HAI S/C TID ACCORDING TO GRBS
- T.PRAZOSIN 5MG PO/OD
- T.THYROXIN 150MCG PO/OD BEFORE BREAKFAST
- NODOSIS 500MG PO/OD
- T.OLKEN TRIO PO/OD
- INJ.AUGMENTIN 1.2GM IV TID
- SYP ASCORYL LS 10ML PO/TID
- T.VYMADA 50MG PO/BD
- T.VYSOV-D 100/10 PO/OD
Advice at Discharge
Dietary Restrictions:
- Fluid Restriction: Less than 1 lit/day
- Salt Restriction: Less than 2-3 gms/day
Medications:
- Inj HAI S/C: 6 units BD 8 AM and 8 PM before food
- Tab Augmentin 625 mg: PO/BD x 3 days
- Tab Lasix 40 mg: BD x 15 days
- Tab Vysov D 100/10: PO/OD x 15 days (1 PM)
- Tab Vymada 50 mg: PO OD x 15 days
- Tab Prazosin 5 mg: PO OD x 15 days
- Tab Olkem Trio: PO OD x 15 days
- Tab Nodosis 500 mg: PO BD x 15 days
- Tab Thyronorm 150 mcg: PO OD to be continued
- Tab PAN 40 mg: PO OD
- Syp Ascoril LS 10 ml: PO BD x 5 days
- T.Shelcal XT: PO OD at 2 PM for 15 days
- Monitor Glucose At Home: Check using a Glucometer at 7 AM, 10 AM, 4 PM, 10 PM
- Follow Up:
- Review to GM OPD SOS
- When to Obtain Urgent Care:
In case of any emergency, immediately contact your consultant doctor or attend the emergency department.
Preventive Care:
- Avoid self-medication without doctor's advice.
- Do not miss medications.
- In case of Emergency or to speak to your treating faculty or for appointments, please contact _____________.
For Treatment Inquiries Patient/Attendant Declaration:
The medicines prescribed and the advice regarding preventive aspects of care, when and how to obtain urgent care have been explained to me in my own language.
Discharge Date Date: 25/10/24
PPM 1: Trunkal obesity and sarcopenia phenotype

 OPD review post discharge 11 days from ICU where she was admitted with severe heart failure secondary to her metabolic syn with diabetes since 12 years.
OPD review post discharge 11 days from ICU where she was admitted with severe heart failure secondary to her metabolic syn with diabetes since 12 years.


[10-11-2024] PA; 95mg/dl, BP 181/79, 92
Before eating BP 152/80, 95
After having breakfast 126mg/dl
PPM 1: 👍
Patient Advocate kindly send her chest X-ray, ecg, echo video from this admission
PPM 1: Deidentified 👍
@43F Diabetes PA also check the two case report links in the description box and let us know if you feel they are fine
Patient Advocate: Okay
CR: @PPM1 they don't have any reports. It is kept by the faculty for the senior dr.
PPM 1: It can be accessed by one of our residents I guess
Patient Advocate: BP 101/84, 127mg/dl
158/74, 100
169/98, 101
133/120, 100
PPM 1: Please share what medications she's taking and mention at what time
PA: Okay
175/89, 98. Before eating - Morning



At night

Sodium bicarbonate and N acetyl cysteine tablets can be stopped.
PA: Vial is insulin bottle taking 2 times per day.
PPM 1: @CR can you help this PA to arrange all the BP data with time today serially also mention the time her BP medications were taken in one single text that you can then use to prompt the LLm to generate a graph.
PPM 1: Share the name of that insulin. What's her last serum creatinine? How much dose?
PA: Test was done at hospital only. We have no pdf or reports with us
PPM 1: 10U twice a day? The insulin looks like water?





 {01-04-2025 14.46] CR: @PPM1sir the patient advocate is asking "should we inject directly or need to mixup any saline water to patient"
{01-04-2025 14.46] CR: @PPM1sir the patient advocate is asking "should we inject directly or need to mixup any saline water to patient"









19/09/2025

PA: Yes
PPM 1: It's there in her case report done by @CR linked in this group's description box.
PA: BP 164/84
CR: [11/10, 8:16 PM] 43F Diabetes PA: I have one doubt why PPM1 told to stop N acetyl med??
[11/10, 8:16 PM] 43F Diabetes PA: That med helps to decrease the creatinine level
[11/10, 8:16 PM] 43F Diabetes PA: It's kidney meds
PPM 1: N acetyl cysteine may not be helping in anything as it's not supported by scientific evidence
CR:
20-11-2024
PA: 86mg/dl, 156/82, 98
PPM 1: 👍
[06-01-2025] PPM 1: Reviewing the patient right now in the OPD @CR
Was alright since her last discharge in November and came once for follow up in December for pedal edema but otherwise was NYHA 1! Was able to walk from the hospital gate to our OPD without any shortness of breath.
The edema subsided in December.
Now complains of chest pain since yesterday
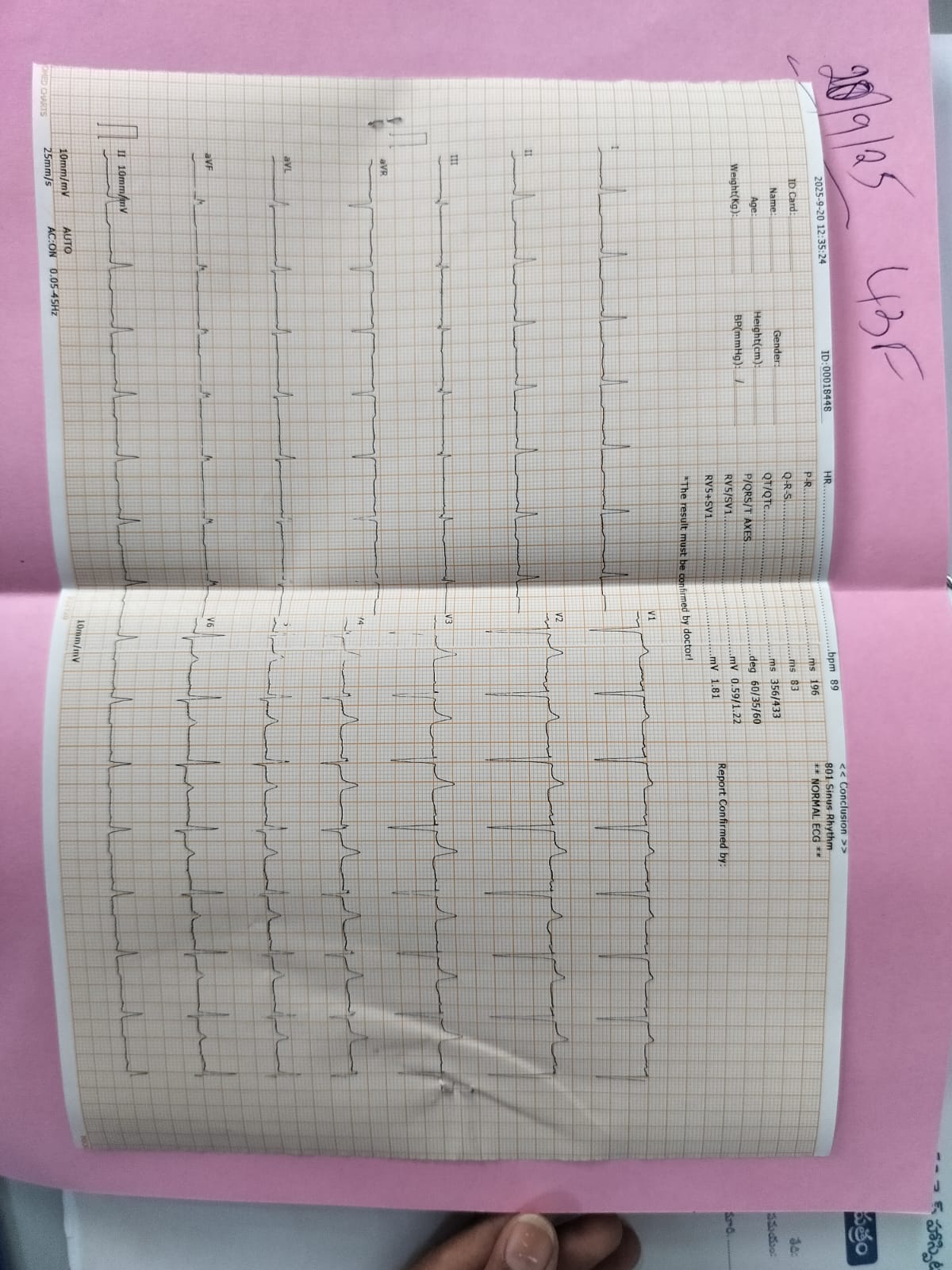
11 March 2025
PPM 1: OPD now:
Reviewing 43F currently in OPD:
In NYHA II also complaining of pruritus over her abdomen
Repeat chest X ray today

ECG done on 11-03-25



[01-04-2025 14:55] PPM 3: Can't comment unless we have patients daily DELSM schedule.
[01-04-2025 16:39] PPM 1: Does she need this injection?
How many has she taken till now? Or this is likely her first?
Please share the deidentified prescription for that injection and please check the events timeline for indicators as to why this may have been prescribed
[01-04-2025 16:41] PPM 1: A student in KMC Warangal has a thesis around this disease where this injection is commonly prescribed and he's studying similar patients such as this with COPD as well as CKD anemia where this injection is often prescribed for renal anemia although again the evidence of it's efficacy is still suspect
[01-04-2025 16:52] CR: PA: "That injection prescribe by Nephrologist for Increament in blood.
Only one she has injected.
Recent blood test hua thaa.
Uskhey baad Dr same injection prescribe Kiya.
Wo Injection gives alot of improvement."
[01-04-2025 17:04] PPM 1: Thanks.
How do we know scientifically that the injection is useful to the patient?
We need to look at trials that have compared similar patients given the same erythropoietin injection vs placebo and then see how much better did the patients receiving erythropoietin do over those receiving placebo.
@Meta AI please share one best randomized controlled trial that looks at the above question of erythropoietin injection efficacy over placebo and share the outcomes in a PICO format taking care to not use any relative percentages but absolute values
[01-04-2025 17:04] Meta AI: One notable randomized controlled trial (RCT) evaluating the efficacy of erythropoietin injection versus placebo is:
Trial: Evolution of Cardiovascular Risk in New Erythropoiesis-Stimulating Agent in Chronic Kidney Disease (EPO-CKD) trial, but a more relevant trial is the "Normalization of Hemoglobin Level in Patients with Chronic Kidney Disease" trial by Parfrey et al. (2005)
PICO (Patient, Intervention, Comparison, Outcome) format:
- P (Patient): Patients with chronic kidney disease (CKD)
- I (Intervention): Erythropoietin injection (epoetin alfa), targeting a higher hemoglobin level (13.0-15.0 g/dL)
- C (Comparison): Placebo
- O (Outcome): Change in hemoglobin levels, quality of life, exercise capacity, and cardiovascular events
Outcomes:
- The erythropoietin group achieved a mean hemoglobin increase of 2.2 g/dL over the placebo group at 12 months
- The erythropoietin group demonstrated improved quality of life and exercise capacity compared to the placebo group
- However, the erythropoietin group had a higher incidence of cardiovascular events (e.g., myocardial infarction, stroke) compared to the placebo group
Please note that while erythropoietin injections can effectively increase hemoglobin levels, they may also carry risks, particularly related to cardiovascular events.
[01-04-2025 17:05] PPM 1: @CR verify if the above findings are true through a Google search for the actual article
[01-04-2025 17:09] CR: Ok sir. 👍
[22-09-2025 15.55] PPM 1: Admitted again with heart failure symptoms recently on 17/9/25


19/09/2025
No comments:
Post a Comment