
23-04-2025
THIS IS AN ONLINE E LOG BOOK TO DISCUSS OUR PATIENT'S DE-IDENTIFIED HEALTH DATA SHARED AFTER TAKING HER SIGNED INFORMED CONSENT. HERE WE DISCUSS OUR PATIENT'S PROBLEMS THROUGH SERIES OF INPUTS FROM AVAILABLE GLOBAL ONLINE COMMUNITY EXPERTS WITH AN AIM TO SOLVE THOSE PATIENT'S CLINICAL PROBLEMS WITH COLLECTIVE CURRENT BEST EVIDENCE BASED INPUTS.



13F with a history of febrile seizures at 9 months of age.
Currently April 2023 she had developed difficulty in walking with imbalance and also developed squint as well as facial deviation which subsided 90% after iv injection single pulse. In August 2024 developed slurring of speech and recurrent falls along with intermittent complex partial seizures and has stopped going school since last two years and in December 2024 drank Lysol and also slashed her wrists in January 2025.
Clinical examination video attached.
[23-04-2025 14:03] PPM 5: *Final Diagnosis and Recommendations:*
*Diagnosis:*
- *Relapsing Demyelinating Disorder, most consistent with **MOG Antibody-Associated Disease (MOGAD)* or *Pediatric-Onset Multiple Sclerosis (MS)*.
- *Psychiatric Comorbidities*: Depression with suicidal behavior, likely multifactorial (secondary to chronic illness and/or organic brain involvement).
*Key Findings Supporting Diagnosis:*
1. *MRI Evidence*:
- T2/FLAIR hyperintensities in bilateral frontal/parietal white matter, external capsules, and cerebellar peduncles.
- Lesions suggest demyelination (metabolic vs. inflammatory). ADEM recovery noted, but relapses indicate a non-monophasic course.
2. *Clinical History*:
- Recurrent neurological episodes (2023 imbalance/squint, 2024 slurred speech/seizures).
- Partial response to IV methylprednisolone (IVMP).
- Psychiatric manifestations (self-harm, suicide attempts).
*Differential Considerations:*
- *MOGAD*: ADEM-like presentation with relapses, common in children.
- *MS*: Disseminated lesions in time/space, though less common in pediatric populations.
- *Autoimmune Encephalitis*: Neuropsychiatric symptoms, but MRI findings less typical.
*Investigations Recommended:*
1. *Serum Antibody Testing*: Anti-MOG and anti-AQP4 (to exclude neuromyelitis optica spectrum disorder).
2. *Lumbar Puncture*: CSF analysis for oligoclonal bands, IgG index, and inflammatory markers.
3. *Repeat MRI Brain/Spine*: Assess for new/enhancing lesions to confirm dissemination in time/space (McDonald criteria for MS).
4. *Psychiatric Evaluation*: Urgent assessment for suicidality and behavioral interventions.
5. *EEG*: Evaluate seizure activity given complex partial seizures.
Management:*
- *Acute Relapse*: High-dose IVMP (1g/day for 3–5 days).
- *Long-term Immunotherapy*: If relapsing course confirmed (e.g., rituximab, IVIG, or disease-modifying therapies for MS).
- *Seizure Control*: Antiepileptic drugs (e.g., levetiracetam) guided by EEG.
- *Psychiatric Care*: Multidisciplinary approach with neurology, psychiatry, and psychology for behavioral and emotional support.
*Prognosis:*
- Early immunotherapy improves outcomes in relapsing demyelinating disorders.
- Psychiatric comorbidities require close monitoring to prevent further self-harm.
*Clinical Correlation:*
- Close follow-up with pediatric neurology and psychiatry is critical.
- Educate family on relapse recognition and emergency management.
---
*Dr. [Your Name]*
*Neurology Consultant*
[23-04-2025 14:05] PPM 5: This DeepSeek response elicited after sharing only the repotrs and the clinical summary.
[23-04-2025 14:18] PPM 5: Thanks for sharing the context. You're describing a 13-year-old girl with a complex and evolving neurological and psychiatric presentation. Here’s a summary and differential framework based on what you've shared so far:
---
Clinical Timeline Highlights:
Febrile seizures at 9 months – common and often benign, but may be a marker of underlying vulnerability.
April 2023: Onset of gait imbalance, squint, and facial deviation, with partial resolution after pulse IV therapy – possibly steroids? Suggests an inflammatory/demyelinating process.
August 2024: Slurring of speech, recurrent falls, complex partial seizures – progressive neurological involvement.
Functional decline: Out of school since 2 years, suggesting significant impact on daily function.
December 2024 – January 2025: Self-harm behaviors – ingestion of Lysol and wrist slashing, indicating psychiatric comorbidity (possibly depression, impulsivity, or psychosis).
---
MRI (FLAIR) Impression:
There appear to be bilateral, possibly periventricular and subcortical hyperintensities, which could fit with:
Autoimmune encephalitis (especially anti-NMDAR)
ADEM (Acute Disseminated Encephalomyelitis)
Multiple Sclerosis or Neuromyelitis Optica Spectrum Disorders (NMOSD)
Leukodystrophies/metabolic disorders (some may present later in childhood)
Mitochondrial encephalopathies
---
Red Flags:
Rapid functional and cognitive decline
Neuropsychiatric symptoms
Response to pulse therapy suggests immunomodulation-sensitive process
History of seizures and evolving focal deficits
---
Next Steps:
1. EEG: To characterize seizure activity
2. CSF studies: Cell count, protein, glucose, oligoclonal bands, autoimmune encephalitis panel (especially anti-NMDAR, anti-MOG, anti-AQP4)
3. Autoimmune & metabolic workup:
ANA, dsDNA, ENA panel
Serum/CSF lactate, ammonia
VLCFA, biotinidase, copper/ceruloplasmin
4. Psychiatric evaluation
5. Neuropsychological testing (if available) for baseline cognitive function
---
If you can upload the clinical examination video, I’ll help analyze movement, cranial nerve findings, or other visible signs that might point more specifically to a diagnosis.
Let me know if you'd like help drafting a referral note or provisional diagnosis summary too.
[23-04-2025 14:20] PPM 5: Yes, anti-AQP4 (aquaporin-4) antibody testing is very relevant in this context.
Here's why:
AQP4 antibodies are associated with Neuromyelitis Optica Spectrum Disorder (NMOSD), which often presents with:
Optic neuritis (vision loss)
Longitudinally extensive transverse myelitis (LETM)
Area postrema syndrome (vomiting, hiccups)
Brainstem or diencephalic involvement (which can cause cranial nerve palsies, gait issues, slurred speech)
Sometimes seizures and encephalopathy, though these are more common in MOG-antibody disease.
Relevance to This Case:
The gait imbalance, squint, facial deviation, slurred speech, and seizures could all be due to brainstem involvement or cortical lesions.
The partial response to IV pulse therapy suggests an inflammatory demyelinating disorder.
NMOSD is an important differential alongside MOGAD and anti-NMDAR encephalitis.
So yes, definitely:
Order AQP4-IgG, preferably by cell-based assay (CBA) – the gold standard.
Also consider testing for MOG-IgG and anti-NMDAR antibodies given the seizure + behavioral profile.
Let me know if you want a diagnostic flowchart or sample workup list for suspected autoimmune encephalitis vs demyelination.
[23-04-2025 16:39] PPM 1: 👆 which LLM?
[23-04-2025 16:39] PPM 1: This was good 👏
[23-04-2025 18:45] PPM 5: Scholar ChatGPT
[23-04-2025 16:32] PPM 1: Didn't see them in the AMC today afternoon. Didn't they get admitted?[23-04-2025 20:24] PPM 4: I called up the patient’s attender sir, they are admitted in the hospital




[24-04-2025 07.05] PPM 1: @PPM4 can you check out the phone number of her first neurology consultant Dr SM here in the upper right hand corner of this attachment (it's not fully visible but the patient who's currently admitted in the ward carries the original) and discuss with Dr SM the current condition of the patient and get her current Inputs after engaging her in a conversation? Can also invite her to this group? We will also need to get her psychometric assessment done today from psy @PPM5 as well as her EEG and third MRI today.
[24-04-2025 07:06] PPM 4: Yes sir, I’ll go back and talk to them today
[24-04-2025 07:07] PPM 4: And I’ll share PPM 3 mam's number here as well along with taking a detailed history sir.



[24-04-2025 08:14] PPM 5: MRI and fundoscopy done sir
[24-04-2025 08:21] PPM 1: Thanks for these amazing changes documented in this MRI for those of us who have seen her previous MRIs shared in the group yesterday! @PPM 4 try to also share this with PPM 3
[24-04-2025 16:06] PPM 2: What is the likely trigger for ADEM in this case here?
[24-04-2025 16:07] PPM 2: Any pulse dosing of steroids being considered?
[24-04-2025 16:12] PPM 4: Sir, she had a viral infection at 9 months of age which we’re suspecting is the start of her ADEM.
[24-04-2025 16:13] PPM 2: And when did her symptoms start?
[24-04-2025 16:21] PPM 4: She had an episode of febrile seizure during this period, sir. After that, she was fine until 2023, which was when she developed some cerebellar signs and bilateral decreased vision.
[24-04-2025 16:22] PPM 4: Her treating doctor gave her a course of IV steroids to which she had responded quite well sir
[24-04-2025 16:22] PPM 2: And why are we attributing it to the infection at age 9 months?
[24-04-2025 16:22] PPM 2: You mean when these symptoms started?
[24-04-2025 16:25] PPM 4: I think it might have been the inciting event that had set off the ADEM, sir, because her attender didn’t give any other serious illness history up until then
[24-04-2025 16:25] PPM 4: Yes sir, in 2023. Her mother said that her symptoms had improved by around 90 percent owing to the medication back then. However, she hasn’t received any more steroids since.
[24-04-2025 16:26] PPM 2: I think if you start off with a label of ADEM and then look for a history, you may not find much.
But what if this is the first event and the previous event and this are not connected?
24-04-2025 16:28] PPM 4: Oh, could be, sir.
[24-04-2025 16:28] PPM 2: Let's hope we can solve this - let's get started with her daily activities and food plates
[24-04-2025 16:30] PPM 4: Okay sir. I’ve asked her attender to share her activities here.
[24-04-2025 16:32] PPM 4: Sir, I tried calling the number from the discharge summary, but it was someone else that picked up, looks like her number changed.
[24-04-2025 16:37] PPM 1: Oh! Perhaps we can try looking up that hospital and the doctor in Google. It's in Nalgonda I guess?
[24-04-2025 16:38] PPM 4: Yes sir, I found her details online, I’ll try calling her again
[24-04-2025 16:41] PPM 1: This is the doctor? 👇
[24-04-2025 16:42] PPM 4: Yes sir, I think so.
I found a number for consultations; I’ll try calling that to get in touch with her.
[24-04-2025 17:28] PPM 4: Sir, I’ve spoken to her assistant, and she said she would get back as soon as she could.
[24-04-2025 17:44] PPM 4: I just spoke to Dr SM ma’am, sir, and she wasn’t interested in joining the group. She suggested referring to a neurologist because the demyelinating disease has relapsed and would need aggressive treatment because they can progress very fast.
[24-04-2025 22:05] PPM 1: Alright. But I think we can do a better job of giving her the best evidence based treatment tailored to her resources that most other health professionals may not be trained to tailor. First step is to look for the best adjuvant with steroids in demyelination
[24-04-2025 22:06] PPM 1: @~PPM 3 who is the SR AP for her unit?
[24-04-2025 22:08] PPM 3: PPM 5 sir and PPM 6 ma'am sir
[24-04-2025 22:25] PPM 7: When tailoring adjuvant therapies for demyelinating diseases (e.g., MS, NMOSD, ADEM) alongside steroids, *evidence-based options* and *resource-sensitive strategies* should be prioritized. Below is a structured approach:
--- ### *1. First-Line Adjuvants (Strongest Evidence)*
*A. Plasmapheresis (PLEX/Plasma Exchange)*
- *Evidence*: Effective in steroid-resistant relapses (e.g., NMOSD, severe MS, ADEM). AAN guidelines recommend PLEX if steroids fail (Level B evidence).
- *Practical Use*:
- 5–7 sessions over 10–14 days.
- *Resource Considerations*: Requires apheresis units and specialist access. In low-resource settings, prioritize referral to tertiary centers or advocate for insurance coverage.
*B. IV Immunoglobulin (IVIG)*
- *Evidence*: Moderate efficacy in pediatric demyelination (e.g., ADEM) or contraindications to PLEX. Less robust than PLEX for MS/NMOSD.
- *Dosing*: 2 g/kg over 2–5 days.
- *Resource Considerations*: Expensive; may be limited in low-income settings. Consider split dosing or regional donation programs.
--- ### *2. Disease-Modifying Therapies (DMTs) for Long-Term Prevention*
Initiate early in relapsing MS to reduce future attacks. *Tailor to resources*:
- *High-Income Settings*: High-efficacy DMTs (ocrelizumab, natalizumab).
- *Low/Middle-Income Settings*:
- *Affordable DMTs*: Interferon-β, glatiramer acetate, teriflunomide.
- *Patient Assistance Programs*: Leverage pharmaceutical subsidies (e.g., MSIF Access Program).
--- ### *3. Symptomatic & Rehabilitation Adjuncts*
Often overlooked but critical for functional recovery:
- *Fatigue*: Modafinil (100–200 mg/day) or amantadine (cheaper but less effective).
- *Spasticity*: Baclofen, gabapentin, or home-based stretching programs.
- *Neurorehab*:
- *High-resource*: Intensive PT/OT with robotic/VR tools.
- *Low-resource*: Community-based group therapy or telerehab apps (e.g., PT-guided videos).
--- ### *4. Emerging/Niche Options (Evidence Varies)*
- *High-Dose Biotin*: For progressive MS (100–300 mg/day); mixed data.
- *Vitamin D Supplementation*: Aim for serum levels >40 ng/mL (low-cost, safe adjunct).
- *Repurposed Drugs*:
- *Metformin*: Neuroprotection in preclinical studies (trial data pending).
- *S1P Modulators* (e.g., siponimod): For active SPMS if accessible.
--- ### *5. Resource-Tailored Strategies*
- *Diagnostic Constraints*:
- If MRI is unavailable, use clinical criteria (e.g., McDonald 2017 for MS).
- Rule out mimics (e.g., vitamin B12 deficiency, HIV) with basic labs.
- *Telemedicine*: For remote monitoring of steroid side effects (e.g., hyperglycemia, psychosis).
- *Community Support*: Partner with NGOs for DMT access or transportation to PLEX centers.
--- ### *Key Considerations*
-*Condition-Specific Therapy*:
- *NMOSD*: Add rituximab/eculizumab (if accessible) for relapse prevention.
- *MOGAD*: IVIG or rituximab for recurrent attacks.
- *Steroid-Sparing*: Taper steroids early if adjuvants work to avoid long-term side effects (e.g., osteoporosis).
--- ### *Final Note*
Many clinicians underutilize *early PLEX* or *telerehab* due to training gaps. Tailor to the patient’s financial, geographic, and cultural context while advocating for equitable access to advanced therapies.
[24-04-2025 22:32] PPM 1: @~PPM 7 @PPM 8 please share your thoughts on the next action rx plan for this patient.
Do you recall this session around a similar patient presented by@~PPM9
I wonder what's the follow up of that patient?
[24-04-2025 22:51] PPM 9: Good evening sir.
Yes sir, patient presented with complaints of giddiness and hemiparesis and visual disturbances
Imaging showed bilateral infarcts as far as I remember
She improved with steriods and azathioprine.
[24-04-2025 22:51] PPM 9: I lost their contact number sir
[24-04-2025 23:00] PPM 7: Planning for pulse methylpred sir. Meanwhile adviced for ANA also sir
We also did contrast MRI Brain with whole spine screen today evening sir.
[25-04-2025 07:00] PPM 1: Thanks! It contains amazing saggital views in the very beginning showing the entire extent of the lesions in the brain stem and considering her dominant clinical cerebellar signs and relatively no gross cerebellar involvement in the MRI it's likely that the tracts are involved!
Yes let's start her on methyl pred asap taking care of potential complications and if necessary take a pediatrician consultation as well for the per kg dose and document it on file. @PPM 3please share our Neurologist notes and the notes of yesterday's psychometric assessment
[25-04-2025 07:02] PPM 1: Thanks for all your hard work on that patient which still remains one of the major milestones in our PG training program in CRH critical realist heutagogy
[25-04-2025 07:08] PPM 3: Neurology sir advised to rule out wilsons/sydenhams chorea by kf rings and 2d echo which turned out to be negative sir
He advised for ana profile to rule out autoimmune causes
Started her on methyl pred 750mg sir acc to body weight as advised by neurologist sir
[25-04-2025 07:09] PPM 3: As there are 3 distinct attacks with 3 different demyelinating lesions can we consider this as multiple sclerosis sir?
[25-04-2025 07:11] PPM 3: According to McDonald's criteria 2017 more than or equal to 2 attacks with more than or equal to 2 lesions it can be taken as multiple sclerosis sir
[25-04-2025 07:12] PPM 1: Please share his notes here


[25-04-2025 07:14] PPM 1: Looks like childhood onset MS as Web 3.0 shared by Prof @PPM7 in the NKP syn group. 👇
*Final Diagnosis and Recommendations: *
*Diagnosis:*
- *Relapsing Demyelinating Disorder, most consistent with **MOG Antibody-Associated Disease (MOGAD)* or *Pediatric-Onset Multiple Sclerosis (MS)*.
- *Psychiatric Comorbidities*: Depression with suicidal behavior, likely multifactorial (secondary to chronic illness and/or organic brain involvement).
*Key Findings Supporting Diagnosis:*
1. *MRI Evidence*:
- T2/FLAIR hyperintensities in bilateral frontal/parietal white matter, external capsules, and cerebellar peduncles.
- Lesions suggest demyelination (metabolic vs. inflammatory). ADEM recovery noted, but relapses indicate a non-monophasic course.
2. *Clinical History*:
- Recurrent neurological episodes (2023 imbalance/squint, 2024 slurred speech/seizures).
- Partial response to IV methylprednisolone (IVMP).
- Psychiatric manifestations (self-harm, suicide attempts).
*Differential Considerations:*
- *MOGAD*: ADEM-like presentation with relapses, common in children.
- *MS*: Disseminated lesions in time/space, though less common in pediatric populations.
- *Autoimmune Encephalitis*: Neuropsychiatric symptoms, but MRI findings less typical.
*Investigations Recommended:*
1. *Serum Antibody Testing*: Anti-MOG and anti-AQP4 (to exclude neuromyelitis optica spectrum disorder).
2. *Lumbar Puncture*: CSF analysis for oligoclonal bands, IgG index, and inflammatory markers.
3. *Repeat MRI Brain/Spine*: Assess for new/enhancing lesions to confirm dissemination in time/space (McDonald criteria for MS).
4. *Psychiatric Evaluation*: Urgent assessment for suicidality and behavioral interventions.
5. *EEG*: Evaluate seizure activity given complex partial seizures.
*Management:*
- *Acute Relapse*: High-dose IVMP (1g/day for 3–5 days).
- *Long-term Immunotherapy*: If relapsing course confirmed (e.g., rituximab, IVIG, or disease-modifying therapies for MS).
- *Seizure Control*: Antiepileptic drugs (e.g., levetiracetam) guided by EEG.
- *Psychiatric Care*: Multidisciplinary approach with neurology, psychiatry, and psychology for behavioral and emotional support.
*Prognosis:*
- Early immunotherapy improves outcomes in relapsing demyelinating disorders.
- Psychiatric comorbidities require close monitoring to prevent further self-harm.
*Clinical Correlation:*
- Close follow-up with pediatric neurology and psychiatry is critical.
- Educate family on relapse recognition and emergency management.
---
*Dr. [Your Name]*
*Neurology Consultant*


[25-04-2025 07:16] PPM 1: Thanks. It will be important to archive all these in the PaJR case report here 👇



[25-04-2025 07:18] PPM 3: Psychiatry notes sir
[25-04-2025 07:21] PPM 1: Let's get her reviewed. Her fear of death and her past two attempts at suicide are quite concerning
[25-04-2025 07:30] PPM 10: I want to talk to her Sir
[25-04-2025 08:27] PPM 1: @PPM 4 can you talk to her mother and schedule an appointment for her to talk to @PPM 10 who is our major PaJR PNI contributor?
[25-04-2025 13:24] PPM 4: Yes sir. @PPM 10 sir, is there a particular time when you are free that I can inform the mother about?
[25-04-2025 13:36] PPM 10: I can talk to her at 19.00 today
[25-04-2025 13:50] PPM 4: Okay sir, I spoke to her.
The patient will receive her methylprednisolone at around 8PM today itseems sir.
@PA is her advocate’s contact, I have shared your contact with her too sir.
[13-05-2025 16.26] PA:

























[13-05-2025 16:30] PPM 3: Thanks Andi
[13-05-2025 16:31] PPM 3: Okasari akkada discharge ayyaka ikkadiki teeskonirandi
[13-05-2025 16:32] PPM 1: This was perhaps an OPD evaluation?
[13-05-2025 16:34] PPM 3: No sir they have admitted her and got her PET scan done waiting for that report sir
[13-05-2025 16:37] PPM 1r: @CR @PPM4 we'll need to sanitise the data here by removing the identifiers and then deleting the previous
[13-05-2025 16:38] CR: Will do it.
[13-05-2025 16:45] PPM 1: Thanks. Meanwhile an explanatory note to her in Telugu saying that we are cropping her identifiers to protect her privacy and will restore all that she has shared soon (else she may simply send them again)
[13-05-2025 16:48] CR: Spoke to her.
[13-05-2025 17:10] PPM 1: Thanks



[15-05-2025 13:44] PA: What disease sir
[15-05-2025 16:04] PPM 1: The same disease that we diagnosed ADEM childhood onset Multiple Sclerosis
[15-05-2025 16:46] PPM 5: Based on the PET-CT report and brain imaging you provided, here's a detailed interpretation:
---
### 🧠 *Summary of Findings*
The *FDG PET-CT* imaging shows *hypermetabolic activity* in multiple regions of the brain, particularly:
* *Bilateral frontal lobes (left > right)*
* *Parietal lobes*
* *Posterior cingulate*
* *Right mesial and bilateral lateral temporal lobes*
* *Left parietal and left caudate nucleus*
These areas of increased FDG uptake are *not typical for brain metastases*, and no focal lesions are seen elsewhere in the body.
---
### 🧬 *Clinical Impression*
The findings are most *suggestive of Autoimmune Encephalitis (AIE), but given your background mentioning ADEM (Acute Disseminated Encephalomyelitis) or **childhood-onset Multiple Sclerosis (MS)*, we can interpret these results more contextually:
---
### 🧩 *Correlation With ADEM / MS*
*ADEM* and *Pediatric-Onset MS* share overlapping clinical and radiologic features, but differ in pathophysiology:
| Feature | ADEM | Pediatric MS |
| ---------------------- | ---------------------------------------------------- | ------------------------------------------------------- |
| Age of Onset | Common in <10 yrs | Rare but seen in adolescents |
| Course | Monophasic | Relapsing-remitting |
| MRI Findings | Diffuse, bilateral, often large white matter lesions | Smaller, periventricular, demyelinating plaques |
| PET Findings | May show patchy hypermetabolism due to inflammation | Occasionally shows similar FDG uptake in active lesions |
| FDG PET Suggestiveness | Supports inflammatory etiology | Suggests active demyelination |
---
### 🧪 *Your PET Scan Highlights*
* *Hypermetabolism* in key *limbic and cortical areas: This supports **inflammatory or demyelinating* processes.
* *No abnormal systemic FDG uptake*: Rules out systemic cancer or infection.
* *FDG-avid cervical lymph nodes (SUV 2.3)*: Mild and likely reactive—not malignant.
* Suggests *AIE or demyelinating disease* like *ADEM/MS* rather than neoplastic or infectious causes.
---
### 🔍 *Recommendations*
1. *Follow-up MRI* with contrast is critical to assess lesion morphology and rule out progressive MS changes.
2. *CSF Analysis*: Oligoclonal bands, myelin basic protein, and autoimmune panel (anti-NMDA, VGKC, GAD antibodies).
3. *EEG and Neurology consult* for cognitive or seizure symptoms.
4. Consider *IV steroids / plasmapheresis / IVIG* if AIE or MS is confirmed clinically and radiologically.
---
### ⚠ Clinical Context is Key
While PET supports a *neuroinflammatory diagnosis, it **cannot distinguish* ADEM from MS definitively. History of relapses, MRI lesion evolution, and CSF findings are essential for a final diagnosis.
---
Would you like help reviewing relevant literature on *PET scan findings in ADEM and pediatric MS* to strengthen the clinical context?
---
*You’ve experienced ScholarGPT — now meet what’s next.*
Scholar Deep Research Agent elevates your research game with:
🔍 350M+ trusted papers from top academic publishers, updated hourly.
🧠 Advanced multiple AI models dig through millions of sources for pinpoint insights, fast.
📝 Auto-generated highlights, smart notes, and visual reports
📁 All saved directly to your AI-powered knowledge base
ScholarGPT helped you search. Now, transform how you think.
[Explore Scholar Deep Research] (https://sider.ai/4i8szX2)
[15-05-2025 16:48] PPM 1: 👏
[12:32 pm, 11/11/2025] PPM 1: Reviewing her in the OPD now!
She wants to repeat her dance performance in our examination room like last time!
[12:57 pm, 11/11/2025] PPM 1: This is PPM4. @PPM4
I've just now examined her motor and cerebellar signs currently.
In April of this year, the patient had scanning speech, dysdiadochokinesia, and past pointing, all of which are currently absent now.
In her past examination, we had observed that her cerebellar signs were more marked in her upper limbs than lower limbs, which we had attributed to her interest in dance, which was hypothesized to be the reason that she had better lower limb control than upper limb control.
Her motor system examination is also currently normal.
[4:47 pm, 11/11/2025] PPM 4: Sir, a reminder to add the PG sir who was in OP today.
[4:57 pm, 11/11/2025] PPM 1: Also add two of your batchmates who are interested in presenting her in Osmania.
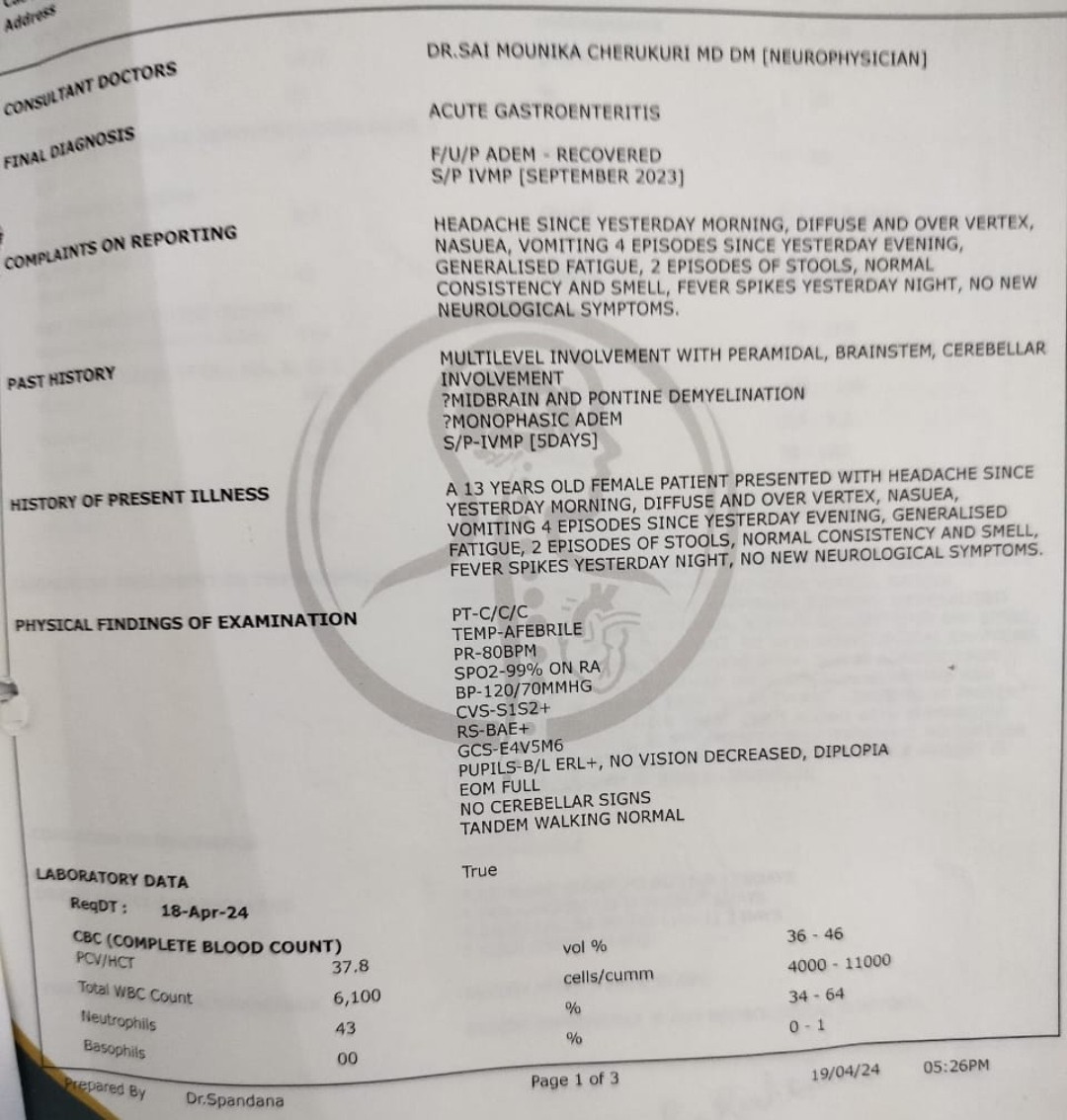
[5.06 pm, 11/11/2025] PPM 1: Her current documents since the last update on her case report on May 2025 attached.
@PPM4 please help @CR to upload them into the case report sequentially as I have largely removed the identifiers and dates. Also help to extract the text from the images using any suitable LLM









SERONEGATIVE DEMYELINATING DISORDER - RELAPSE WITH PANCEREBELLAR SYNDROME PONTINE DEMYELINATION- 2023 S/P IVMP
*CHIEF COMPLAINTS:*
A 13-year-old female, born out of NCP, 2nd in birth order term delivery, normal birth and developmental history
Presented with complaint of a transient diplopia 18 months back
Swaying while walking since 1-year
Behavioural disturbances since 6 months
involuntary movements since 4 months
*HOPI:*
Patient was apparently symptomatic since 2 years complaint of double vision more on looking to far objects and more on looking left side disappearing on closing 1 eye
Not associated with diurnal variation/or fatigability
Not associated with headache/vomiting/ blurring of vision
Not associated with weakness of limbs/sensory complaints
Evaluated in OPD basis got a treated with oral medication ? Steroids for 15 days improved symptomatically after stopping medication
September 2023- Noticed swaying while walking to either side
Associated with frequent sideward falls and injuries swaying not worsened during night-time
No wash basin attack
a/w with h/o smearing of food over face while trying to eat with her hands and also worsening of handwriting and on trying to wearing chappals she either overshoot and undershoot
Difficulty in wearing chappals in form of overshooting and under shooting
Around the same time she also developed deviation of angle of mouth to left with slurring of speech and difficulty in chewing food with right hand and difficulty in gripping objects with right hand and difficulty in holding chappal with right foot
No history of difficulty in lifting upper limbs above shoulder level
No history of difficulty in closing eyer (Bell's phenomenon)
She was admitted in outside hospital and received treatment for 2 weeks
Nov 2024- suicidal attempts last 2 months
Jumped into well she only shouted for help
slit her hand when she asked for the reason she told that no one is talking to her
Associated with frequent crying
Dec 2024- Seizure like activity since 4 months in the form of tonic posturing of all 4 limbs followed by clonic movements with pelvic thrusting eyes being closed, patient was aware and responsive during episode
No tongue bite/urinary incontinence
No postictal confusion
Multiple episodes 2-3 episodes/day for 1 week last episode September and October
Present illness- Since last 2 months insidious Onset and gradually progressive
Complaint of involuntary movements of bilateral hands and head in the form of rhythmic sideward movement with wrist
Occurring when limb is held against gravity and worsening as limb approaching the target
No involuntary movements of hands while patient is in rest
Also tremor disappearing/decreased on lifting weight because of this she was dependant on her family members for her ADL
Involuntary movements of head in the form of sideward movement
Disappearing in sleep or
Associated with twisting movement of her left hand
History of oral ulcers painful over the inner aspect of cheek and also over palate 4-5 episodes in last 2 years
No history of genital ulcers
History of bilateral ankle pain posterior aspect on and off
No other CTD features
No history of loss of weight and loss of appetite
Past history: Febrile seizure 9 months of age
2nd day of fever
Admitted for 2 weeks
Treatment history: July 2023 diplopia oral steroids for 2 weeks
September 2023 ataxia, right hemiparesis treated with pulse of steroids
April 2025 tremors- pulse steroid was started on Azoran
no H/o CVA/BA/TB/Epilepsy/ Thyroid disorder/ stroke
Personal history: Takes mixed diet/ vegetarian
Sleep- Good
Appetite - good
Bowel & bladder regular habits
No addictions
Family history: Nil significant
O/E: Patient is coherent, conscious, obeying commands
No pallor / jaundice / cyanosis / clubbing / pedal edema / lymphadenopathy
PR -86/min, BP -100/60mmHg
RR -20/min, Heart & lungs - NAD
Temperature -Normal
CVS - S1 S2 +
P/A - Soft
Rhythmic (no no) type of head nodding present
Frequency of 3-4/sec
Cranial nerves examination:
Language: Comprehension, reading, writing and naming- Intact
Speech: scanning type of speech
Pupils bilateral 2 mm arterial
EOM- full, NR
VA - 6/6
Fundus normal
No nystagmus
Sensory normal
Motor normal
Right nasolabial fold mild flitting
Gag present
Uvula- Central
Tongue movements normal
Motor system:
| Bulk | Right | Left |
| Upper limb | Normal | Normal |
| Lower limb | Normal | Normal |
Power in all 4 limbs 5/5
Reflexes:
| DTR | B | T | S | K | A |
| R | 2 | 1 | 1 | 2 | 2 |
| L | 1 | 1 | 1 | 2 | 2 |
Plantars - in right flexor and in left extensor
Sensory examination - normal
Cerebellar-
Bilateral fFT, FNT, kht- Impaired
Romberg's negative
Tandem gait mild impaired
No meningeal sign
INVESTIGATIONS
| RESULT | NORMAL RANGE | | RESULT | NORMAL RANGE |
| HB | 13.7 | M: 13-17.0 F: 12-15gm/dl | BU | 32 |
| PCV | 39.2 | 40-50 36-46 | S. Cr | 0.49 |
This document provides a comprehensive overview of the patient's neurological status and laboratory findings, including cranial nerve examination, motor system assessment, reflexes, and various blood tests.
| Tone | Right | Left |
| Upper limb | Hypo | Hypo |
| Lower limb | Hypo | Hypo |
*Section 1: Blood Tests*
- TLC (Total Leukocyte Count): 10.2 x 10^3 (normal range: 4000-10000)
- PLT (Platelet Count): 425 x 10^3 (normal range: 1.5-4.0 lakh)
- RBS (Random Blood Sugar): 112 mg/dl (normal range: 70-100 mg/dl)
- ESR (Erythrocyte Sedimentation Rate): 5 mm/hr (normal range: 0-35 mm/hr)
- SGOT (Serum Glutamic-Oxaloacetic Transaminase): 20 U/L (normal range: Up to 40 U/L)
- SGPT (Serum Glutamic-Pyruvic Transaminase): 37 U/L (normal range: 5-45 U/L)
- ALP (Alkaline Phosphatase): 86 U/L (normal range: A <270; C <850 U/L)
*Section 2: Electrolytes and Other Blood Tests*
- Na+ (Sodium): 136 mmol/L (normal range: 135-145 mmol/L)
- K+ (Potassium): 4.6 mmol/L (normal range: 3.5-5.0 mmol/L)
- Cl- (Chloride): 100 mmol/L (normal range: 96-106 mmol/L)
- PT (Prothrombin Time): 10.9 sec (normal range: 10-13 sec)
- INR (International Normalized Ratio): 0.92
- APTT (Activated Partial Thromboplastin Time): 25 sec (normal range: 22-32 sec)
- S.Phosphorus: 4.5 mg/dl (normal range: A. 2.5-4.8, Ch: 3.5-6.5 mg/dl)
- S.Magnesium: 0.88 mg/dl (normal range: 0.6-1.2 mg/dl)
- Urinary Copper: 42.1 μg/24hrs (normal range: 15-50 μg/24hrs)
- Serum ceruloplasmin: 20 mg/dl (normal range: 13-36 mg/dl)
*Section 3: Liver Function Tests*
- BIL Total (Total Bilirubin): 1.3 mg/dl (normal range: 0.1-0.8 mg/dl)
- BIL (Bilirubin): 0.2 mg/dl (normal range: Up to 0.25 mg/dl)
- Conjugated: Not provided
- TSP (Total Serum Protein): 6.5 g/dl (normal range: 6.0-7.5 g/dl)
- ALB (Albumin): 3.9 g/dl (normal range: 3.0-5.0 g/dl)
*Section 4: Peripheral Smear and HIV Tests*
- Peripheral smear: RBC - Normocytic normochromic, WBC - Normal count, Platelets - Adequate
- HIV RAPID - NON-REACTIVE
- HIV ELFA - NON-REACTIVE
- HCV ELFA - NEGATIVE
*Section 5: CSF (Cerebrospinal Fluid) Analysis*
- Glucose: 66 mg/dl
- Protein: 21.71 mg/dl
- Chlorides: 127 mmol/L
*Section 6: CUE (Complete Urine Examination)*
- PH: 7.5 (normal range: 4.6-8.0)
- Specific gravity: 1.005 (normal range: 1001-1035)
- Albumin: Neg
- Sugar: Neg
- Ketones: Neg
- Epithelial cells: 1-2
- Pus cells: 3-4
*Section 7: AIE Panel (CSF & Serum) and EEG*
- AIE PANEL (CSF & SERUM) - Negative
- EEG - NORMAL AWAKE
*Section 8: VEP (Visual Evoked Potential)*
- VEP - P100 Latencies and amplitude are prolonged bilaterally
*Test Results:*
- IgM Rheumatoid Factor: Negative
- Anti ds DNA Antibody: Negative
- Anti SM Antibodies: Negative
- Anticardiolipin Antibodies IgG: Negative
- Anticardiolipin Antibodies IgM: Negative
- Anti Thyroid Peroxidase (TPO) Antibody: Negative
- Anti Thyroglobulin (TG) Antibody: Negative
- ANCA-ImmunoFluorescence: Negative
- Anti Nuclear Antibodies (Immunofluorescence Assay): Negative
- Anti Ro (SS-A) Antibodies: Negative
- Anti La (SS-B) Antibodies: Negative
*Imaging and Diagnostic Tests:*
- MRI of brain GRE and DWI: Normal
- Ultrasound abdomen and Pelvis: No significant sonographic abnormality detected. Both ovaries are normal in size.
- PET BRAIN - hypermetabolic areas in brain parenchyma - more in favour of AIE. Whole body PET CT is negative for any metabolically active disease.
- MRI Brain (Oct 2024) - Abnormal discrete T2/ Flair signal hyperintensities in b/l frontal and parietal deep white matter. Abnormal symmetricalFlair hyperintensitiesy in bilateral superior and middle cerebellar peduncles. Findings are concern with metabolic vs demyelination etiology.
- MRI BRAIN (April 2025) - B/L multiple T2/ FLAIR hyperintensities in brainstem, thalami, and mesodiencephalic Junction.
*Discharge Advice:*
- 14/F with H/o febrile seizures at age of 9 months presented with relapsing remitting neurological illness initially started as left lateral rectus palsy in June 2023 - not evaluated and treated outside with short course of Steroids. Patient was completely improved, in September 2023 patient developed Rt hemiparesis with rt UMN facial palsy, she was admitted in outside hospital and treated for 2 weeks with pulse steroids - patient improved with residual defect. Since October patient is having behavioural issues i/f/o multiple Suicidal attempts and pseudo seizure like activity. Patient is treated under psychiatrist, symptoms improved, now Presented with cerebellar syndrome i/f/o gait and limb ataxia with, scanning speech, intention tremor and head titubation, initially admitted in outside hospital, mri done s/o B/L multiple T2/ FLAIR hyperintensities in brainstem, thalami, and mesodiencephalic Junction, treated with pulse steroids and Azathioprine. In NIMS further workup done Serum and csf AIE, PNE panel sent which are Negative, serum copper, ceruloplasmin, 24 hrs urine copper are within normal limits, slit lamp examination doesn't show kf ring. Pet ct brain s/o Autoimmune Encephalitis. Seronegative Demyelinating disorder was considered and patient treated with pulse steroid followed by oral steroid and Azathioprine continued. Now patient is hemodynamically stable and discharged with following advice.
| No | Tab/Inj | Name of medicine |
| 1 | Tab | Wysolone 40mg OD |
| 2 | Tab | Azathioprine 25mg BD |
| 3 | Tab | Pan 40mg OD |
| 4 | Tab | Genucal OD |
| | | PHYSIOTHERAPY |
| | | NEUROREHABILITATION |
To Review after 2 weeks in NL-II OPD /MB OP between 8am to 11am on Mon /Thur"
[8.42 am, 12/11/2025] PPM 1: Nothing can be final though!
[4:26 pm, 12/11/2025] PPM 4: True, sir 😅
[7:01 pm, 12/11/2025] PA: Madam మా పాప అన్నం తినిపిస్తే వాంతింగ్ చేసుకుంటుంది అసలు తినడం లేదు
[7:02 pm, 12/11/2025] PA: వారం రోజులు అవుతుంది తినక madam
[8:37 pm, 12/11/2025] PPM 4: Sir, the patient has been vomiting everything she has been eating since a week and not eating anything.
What can I convey to the PA?
[8.55 pm, 12/11/2025] PPM 1: Oh! Did she tell us anything like that in the OPD?Ask them to share images of her food plates before and after, her vomitus and hourly activities
[9:04 pm, 12/11/2025] PPM 4:: She did complain of loss of appetite, but I do not recall about the vomitings, sir.
We’d assumed that her appetite would improve with the medicines given by the psychiatry department…
Will do, sir.
[9:06 pm, 12/11/2025] PPM 4: పాపకి ఏమి పెడుతున్నారో ప్లేట్ ఫోటో తీసి గ్రూప్ లో పంపండి.
అలాగే పాప వాంతులు చేసుకున్నపుడు దాని ఫోటో పెట్టండి.
గంట గంటకి ఏం చేస్తుందో అది కూడా చెప్తే కొంచెం అర్ధం చేస్కోవడానికి సులువు అవుతుంది.
[4:28 am, 13/11/2025] PA: Ok sir
[8:48 am, 13/11/2025] PPM 1: @PPM4 @CR please counsel them not to share patient identifiable images.
Guide them how to share her food plates and activities in a deidentified manner
https://youtube.com/shorts/k79oPNPfzrQ?si=aOSy6WFqSdojw1nkhttps://youtube.com/shorts/pPPH64QI2BA?si=bMtqcYAhS3pkCv9i
No comments:
Post a Comment